
Remember me
There were 220 patients enrolled in the study; on average, each practice included 7.93 patients (minimum: 0, maximum: 36). Overall, women accounted for 63.6% of patients, and the patients’ mean (SD) age was 52.1 (17.9) years (Table 1). In total, 132 patients (60%) had uncontrolled asthma on the basis of an ACQ score of 0.75 or higher (Fig. 1). Women were at greater odds of having uncontrolled asthma (OR, 1.88; 95% CI, 1.01–3.50; p = 0.046), and odds of having uncontrolled asthma decreased with age (OR, 0.98; 95% CI, 0.96–0.99; p = 0.009). Individuals with lower socioeconomic status were at greater odds of having uncontrolled asthma (OR, 2.65; 95% CI, 1.09–6.44; p = 0.031).
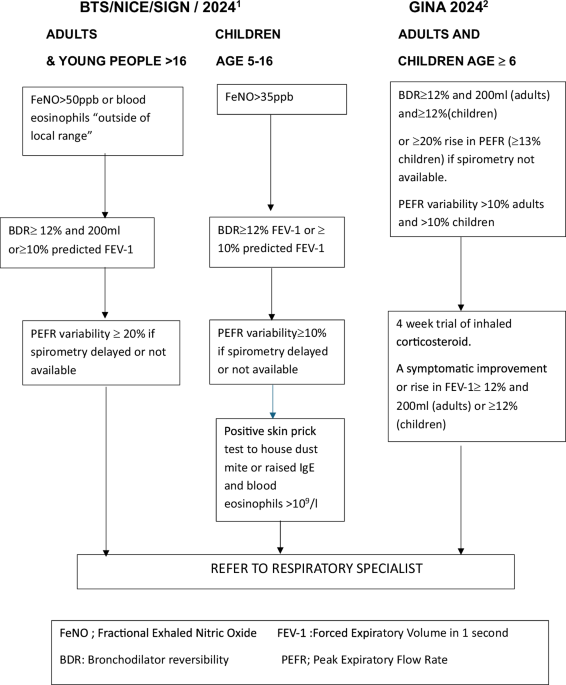
Fig. 1: Distribution of guideline-based management suggestions provided by the AsthmaOptimiser tool for patients with controlled versus uncontrolled asthma.
Total population = 220. Left: patients with controlled asthma (n = 88, 40%). Right: patients with uncontrolled asthma (n = 132, 60%). ICS inhaled corticosteroids.
Table 1 Descriptive statistics of patients in the CAPTURE study.Of the 132 patients with uncontrolled asthma, 85 patients (64%) had modifiable factors that could be addressed during the consultation to optimise the patient’s asthma control (e.g., addressing inhaler adherence or considering an increase in the patient’s inhaled corticosteroid dose). Referrals to a specialist were advised for 45 patients with uncontrolled asthma, of whom 2 patients were already receiving specialist care (Fig. 1). The 2 most frequently reported reasons for referral recommendations occurred in patients with uncontrolled asthma and were adherence issues (n = 25 [58.1%]) and worsening of asthma symptoms at work (n = 25 [58.1%], Table 2). Only 8 of 45 patients with uncontrolled asthma identified for a referral were eventually referred after the consultation in which the AsthmaOptimiser was used, often after having an additional consultation. These 8 patient referrals were made because of persistent shortness of breath, decreased lung function, symptoms after a change in medication, adverse effects from medications, lung attack or pneumonia, nasal polyps, persistent symptoms, and the results of a sleep apnoea test (in 2 patients). Reasons for non-referral are described in Supplement S1.
Table 2 CAPTURE study underlying reasons for advice to schedule a specialist referral.Patients with uncontrolled asthma experienced higher levels and greater odds of work productivity impairment as measured with the WPAI tool (OR, 1.05 per % increase in reduced productivity; 95% CI, 1.03–1.09; p < 0.01) and higher levels and greater odds of impairments in their daily activities (OR, 1.07 per % increase in impairment; 95% CI, 1.05–1.09; p < 0.01; Fig. 2).
Fig. 2: Work productivity and activity impairment in patients with controlled versus uncontrolled asthma.
Work productivity impairment (%) indicates how much work was missed because of health problems and how much work time was impaired while working. Activity impairment (%) indicates impairment in daily activities, irrespective of work, due to health problems. Bar plots show mean and standard deviation.
Mean (SD) bEOS counts for patients with controlled versus uncontrolled asthma were 258 (182) cells/µL and 220 (159) cells/µL, respectively. Patients with uncontrolled asthma were not at greater odds of having a higher bEOS count than patients with controlled asthma (OR, 0.39; 95% CI, 0.06–2.59; p = 0.32).
Usability resultsA total of 33 GPNs and 1 general practitioner participated in the qualitative survey concerning feedback on the AsthmaOptimiser tool. The GPNs were all women, and the general practitioner was male. The respondents’ mean (SD) age was 46.5 (9.4) years, and 11 respondents had missing data. The mean (SD) length of working experience was 11 (8.9) years, with 16 respondents having missing data. The mean (SD) number of hours worked per week for the providers was 25.9 (6.23) hours, with 12 respondents having missing data.
General feedback obtained from the face-to-face interviews with the healthcare providers was grouped as follows: (1) perceptions of the tool before and after use, including positive and negative feedback; (2) AsthmaOptimiser content; and (3) areas of improvement. Prior to using the tool, respondents provided insights about the potential benefits of the AsthmaOptimiser. They felt the tool could be a good addition to asthma consultations, a way to obtain advice for treatment, a way to get advice based on input, and a way to gain insights into whether the patients were doing as well as the providers thought they were. A comment not directly related to the tool addressed current issues that providers face, specifically that it was hard to create an overview of patients with asthma, help patients keep proper control of their asthma, and not have influence on whether their patients come in for annual reviews.
Feedback from providers indicated that they found it easy to log in to the AsthmaOptimiser, the guidance was clear, and patients could complete the ACQ-623 themselves. The most frequent negative feedback was that the tool was time-consuming and could not store all patient data (Table 3). Some of the practitioners had difficulty finding information and felt it was difficult to navigate between areas within the AsthmaOptimiser tool.
Table 3 AsthmaOptimiser usability: feedback from 14 responders.Half of the respondents who provided feedback on the AsthmaOptimiser content identified the inability to add free text to fields marked “other” and requested the inclusion of more follow-up questions (e.g., type of work, how many hours worked, or asthma triggers; Supplemental Table S2). It is worthwhile to note that such free text boxes were not included due to the possibility of writing identifiable patient information in these boxes, which would put additional General Data Protection Regulation (GDPR) requirements on the tool. Additionally, because the AsthmaOptimiser was hosted on AstraZeneca servers and required them to report any adverse events, the option for adding free text was not included in the development. Following user feedback and the transfer of the tool outside AstraZeneca, this has been added to the tool. The respondents also raised questions about the order of some of the questions. For example, questions on exacerbations and lung function tests came before the inhaler technique section.
The respondents also inquired about expanding the amount of information gathered on medication use questions to get a clearer perspective on patient adherence and entering inhaler prescriptions and the number of inhalers patients used. The respondents also noted inconsistencies in how single inhaler prescriptions and the number of inhalers used per year were recorded. Each prescription was interpreted by the tool as 1 inhaler, whereas many patients often pick up multiple inhalers on a single prescription. Another limitation involved a video on inhaler technique. Sometimes, the video worked well; however, in some cases, it stopped working. Overall, the nurses felt that the tool and the advice it provided were useful.
Providers also reported their appreciation of the advice to lower the dose of inhaled corticosteroids. This advice helped 1 provider think about this issue and made it easier to convince the patient to lower their medication dosage. Another provider shared that the suggestions from the AsthmaOptimiser about increasing the dosage of inhaled corticosteroids were seen as a confirmation of their own decision-making abilities. Additional comments about the content focused on receiving more information about ACQ-6 scores and interpretation of or advice about the results, identifying challenges with accounting for medications that started halfway through the year and the difficulty of transitioning to the risk assessment.
Provider feedback on areas of improvement overlapped with comments made about the usability and content of the tool (Supplemental Table S3). A few providers indicated they were waiting for additional features, e.g., self-management plan and traffic light functionality to identify important items to discuss with patients. Discrepancies between data stored in electronic medical records and answers to questions (e.g., smoking may have been a trigger, but the patient’s medical record indicates the patient smokes, which was not true) was another concerning issue raised, along with suggestions to revise the risk factor assessment questions.
Comments (0)