
Remember me






This study used a vignette-based method to generate descriptions of treatment scenarios with several treatment-related attributes [26], and used the time trade-off (TTO) method to elicit health utility values of these scenarios. We recruited patients with T2DM from eight cities in China. The sample was broadly consistent with Chinese patients with T2DM with regard to age and sex distribution. This study has been reviewed and approved by the Academic Ethics Committee at Tianjin University (no. TJUE-2023-206). Informed consent was obtained from all study respondents before the interview. This study also complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [27] and Checklist for Reporting Valuation Studies of Multi-Attribute Utility-Based Instruments (CREATE) [28] (Appendix Tables 1, 2).
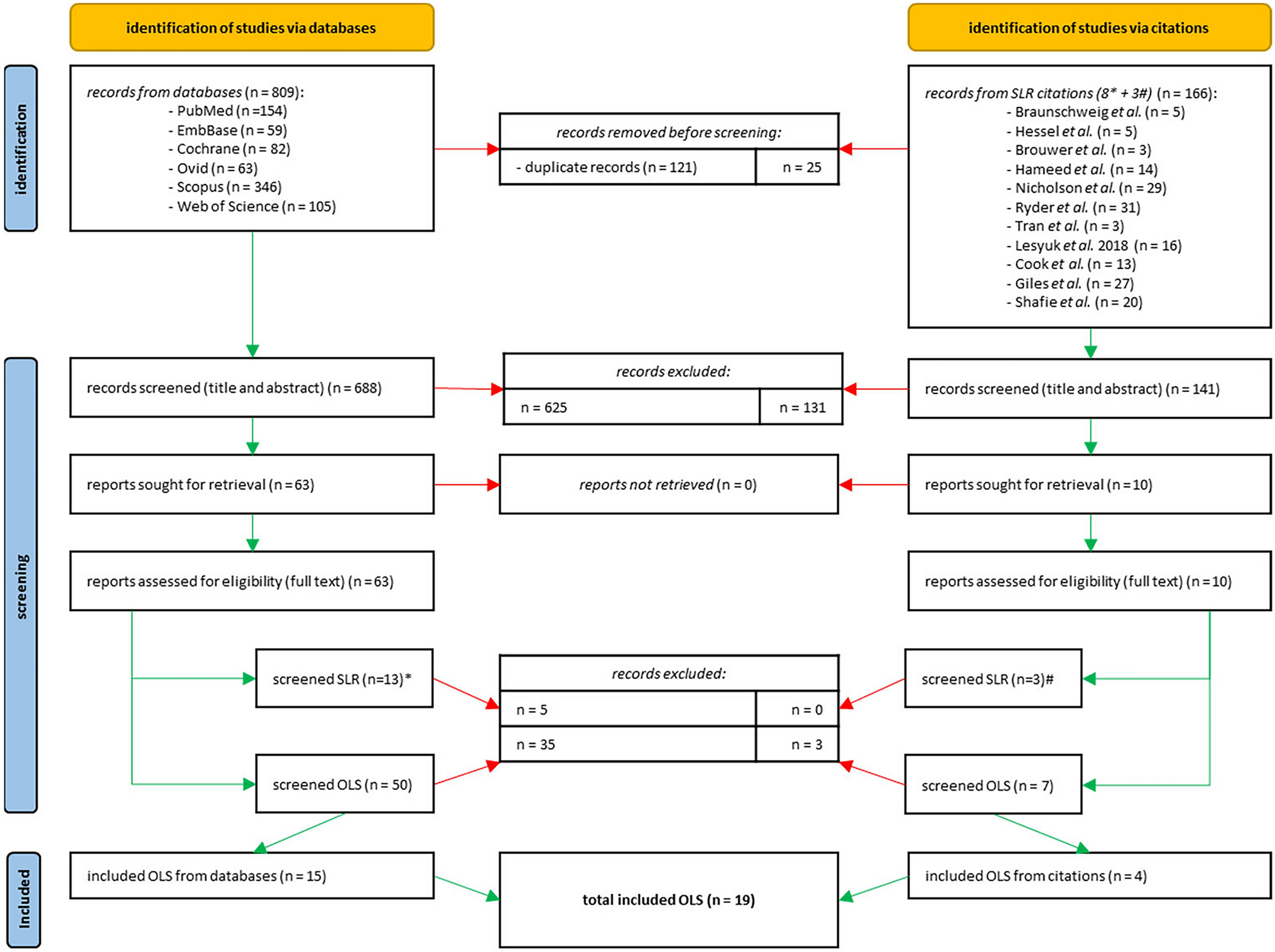
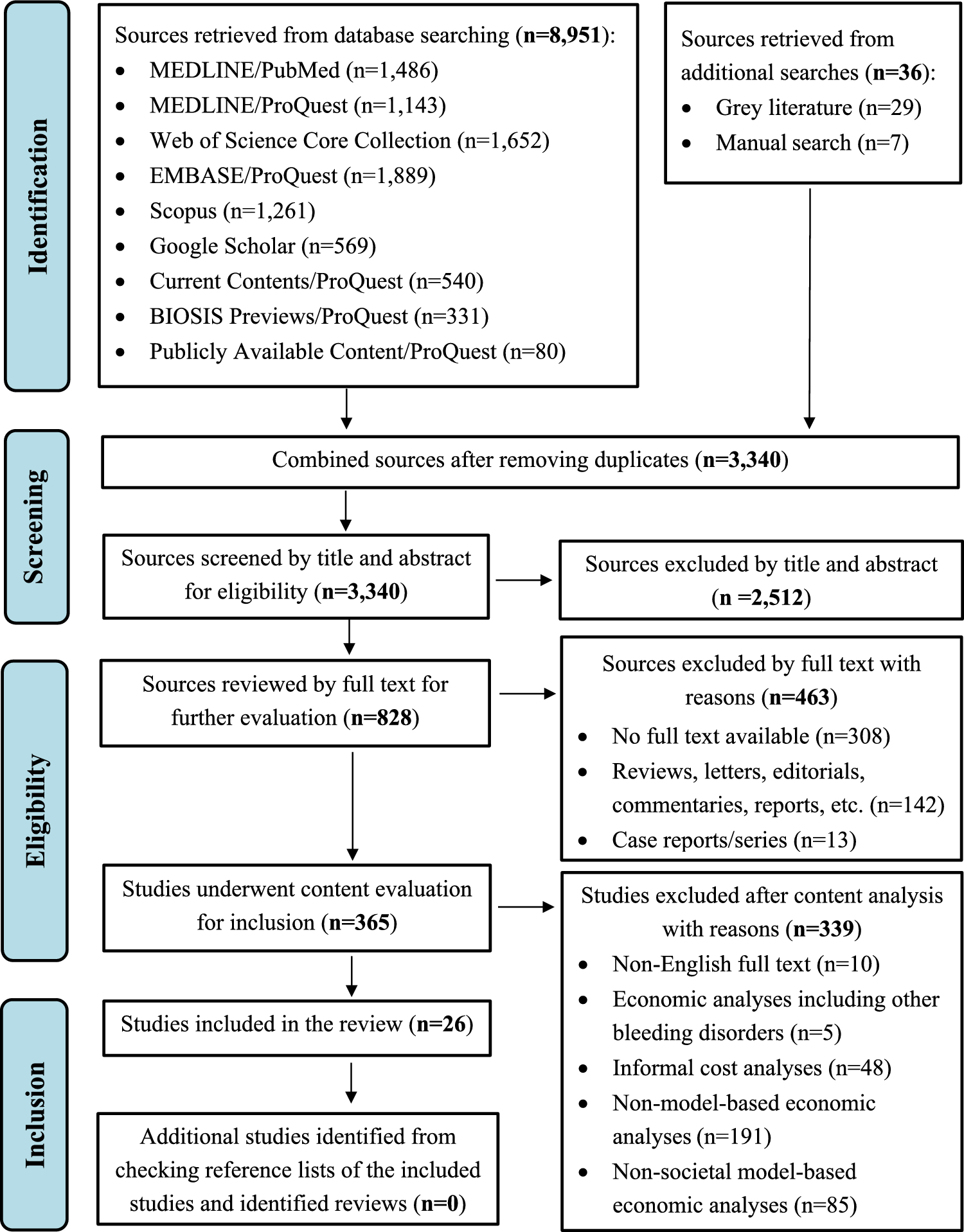
2.1 Health State DevelopmentThe health states were drafted and refined based on a comprehensive process including a literature review, interviews with patients and clinicians, clinical guidelines and prescribing information, and a pilot study. First, we conducted a systematic literature review focusing on the disutility of treatment-related attributes for T2DM [12]. Briefly, we conducted a literature search in Medline (Ovid), Embase, Cochrane Library, PsycINFO, EconLit, and CINAHL (EBSCOHost) databases with keywords of T2DM and disutility value. In this review, eight treatment-related attributes (weight change, dose frequency, gastrointestinal side effects, dose flexibility, administration requirement, injection site reaction, fear of hypoglycemia and HbA1c levels) assessed by nine relevant studies were identified [13,14,15,16,17,18,19, 22, 23]. More detailed information on the review can be found elsewhere [12]. Second, qualitative interviews were conducted with patients with T2DM (N = 16) and clinicians (N = 7) using a semi-structured interview protocol. Participants were asked to identify which attributes were the most important to them during the treatment process. Qualitative information provided by patients and clinicians was used to inform the development of health state descriptions. Third, the descriptions of health states, e.g., the definition of severe and nonsevere hypoglycemia, dose frequency of injections and symptoms of injection site reaction, were refined based on clinical guidelines and prescribing information to ensure clarity and accuracy. Finally, 42 general public respondents were involved in the pilot study using convenience sampling. Each respondent was asked to complete the pilot interview under the supervision of the investigator, and they did not appear to have difficulty understanding the task or distinguishing among the health states. Therefore, no additional revisions were made to the health states before their use in the main study.
The final set of four selected injection treatment-related attributes were hypoglycemia (severe, nonsevere), dose frequency (three times daily, twice daily, once daily, and once weekly), flexibility (need to be carried with the patient on short trips, not need to be carried with the patient on short trips) and injection site reaction (with, without) among which the two attributes of dose frequency and flexibility had a binding relationship (Table 1). Once weekly injection does not need to be carried with the patient on short trips, while the other three levels require carrying for short trips. This design could generate a total of 16 (2 × 3 × 2 + 2 × 1 × 2 = 16) states. The descriptions of all health states are also presented in Table 1.
Table 1 Attribute, level and description of health state2.2 Health State ValuationA total of 150 representative health states among all potential combinations were generated based on the balanced overlap method using Lighthouse Studio 9.15 from Sawtooth Software. These 150 health states were then allocated into 30 blocks, and each respondent was assigned one of 30 blocks (5 TTO tasks). Two additional fixed tasks, e.g., the mildest state (nonsevere hypoglycemia, once weekly injection does not need to be carried with the patient on short trips, without injection site reaction) and the worst state (severe hypoglycemia, three times daily injection need to be carried with the patient on short trips, with injection site reaction), were also included. Therefore, a total of seven TTO tasks (five randomly selected tasks and two fixed tasks) were asked for each respondent.
Each TTO task began by choosing between a health state describing a treatment scenario for 10 years (choice A) or full health for 10 years (choice B) (Fig. 1a). Typically, the latter was preferred. Respondents who preferred living in a treatment health state for 10 years (choice A) or who were indifferent between the alternatives (choices A and B are about the same) were considered irrational and excluded from the analysis. Then, respondents were asked to choose between living with the treatment health state for 10 years or die immediately (Fig. 1b). Health states of worse than death are unrealistic and rare in this therapeutic area, therefore, respondents who preferred to die immediately (choice B) or who were indifferent between the alternatives (choices A and B are about the same) were also considered impossible and excluded from the analysis [18, 23]. After these two quality control processes, a bisection step was used, and respondents were asked to choose between living with the treatment health state for 10 years or full health for 5 years (Fig. 1c). The time in full health was then made shorter if it was preferred or longer otherwise. One-year steps were used unless a change in direction was needed, and the smallest trading increment was half-year. Finally, the respondents’ indifference point was located by varying the time in full health (x, 0 ≤ x ≤ 10), and the utility value of each treatment health state was calculated as x/10 (0 ≤ utility value ≤ 1).
Fig. 1
a Example of TTO task. b Example of TTO task. c Example of TTO task
2.3 Study SamplePatients with T2DM were recruited from eight cities (Beijing, Guangzhou, Shanghai, Baoding, Chongqing, Jiujiang, Mianyang, and Wuhan) to achieve sufficient geographical spread and varied economic development levels in China. Quota sampling was used to ensure that the age and sex distribution of the sample resembled those of the Chinese patients with T2DM [2]. Taking into account the requirement of at least 25 TTO observations per health state to result in robust model estimation and the requirement of subgroup analysis, the target sample size was 400 [29, 30]. All respondents were required to be: (1) age ≥ 18 years, (2) diagnosed with type 2 diabetes ≥ 3 months by a recognized medical professional (patients were required to show proof of diagnosis or medication packaging during the videoconference), (3) were literate and had no disease that limited cognitive function, and (4) gave informed consent.
2.4 Data CollectionOnline face-to-face interviews were used for data collection. Recruitment of the respondents was conducted through a professional online panel company and one interviewer was involved during the interview with each respondent. In each of the selected cities, all the interviewers were led by a local lead investigator and supervised by the principal investigator. Before the beginning of data collection, interviewers attended an online training to ensure equivalent task understanding, iterative procedures, and interactions with respondents. Eligibility for formal survey administration required all interviewers to complete TTO practice tasks, which were assessed by the principal investigator to ensure methodological compliance. The interview started with the respondent completing the quota questions (e.g., age and sex) and providing a series of socio-demographic characteristics (e.g., education level, marital and employment status). Second, all respondents were asked to report their own health state on the EQ-5D-5L and then complete seven TTO tasks. Last, respondents provided diabetes-related information (e.g., current treatment, number of medications and diabetes-related complications). A quality control check was conducted, where respondents were required to correctly identify diabetes therapeutics from a medication list including: metformin, repaglinide, acarbose, dapagliflozin, liraglutide, and distractors amlodipine and bisoprolol. Selection of either nondiabetes therapeutics (amlodipine or bisoprolol) resulted in exclusion. All interviews were conducted from October 2023 to January 2024.
Data collected by the interviews were directly excluded from the analysis if they: (1) contained any missing data, (2) provided a wrong answer to the quality control question of choosing T2DM drugs, and (3) failed to pass TTO quality control processes.
2.5 Data AnalysisDescriptive analyses were first conducted to present the respondents’ characteristics. The utility value for the self-reported EQ-5D-5L health state was calculated using the China value set [31]. Ordinary least square (OLS), fixed effects (FE), and random effects (RE) models were used to estimate disutility values of treatment-related attributes:
$$_=\alpha +\sum_\sum___+\epsilon ,$$
(1)
where \(_\) represented the disutility value; \(\alpha\) represented the intercept (i.e. the mildest state in our study); \(_\) represented five dummy variables indicating the health state described by dimension \(d\) at level \(l\), except the mild level of each dimension (for reference); \(_\) represented the coefficient representing the estimated disutility value of having problems on dimension \(d\) at level \(l\); and \(\epsilon\) represented the error term. Considering each respondent completed seven TTO tasks, in addition to the OLS estimator with cluster-robust standard errors, the FE and RE models were also considered to account for the panel structure in the data [32].
The disutility value was used as the response variable and each level of the attribute as predictor variable. The preferred models for TTO were selected based on the Breusch Pagan LM test, Hausman test, and the goodness of fit of the model using the Akaike information criterion (AIC) and Bayesian information criterion (BIC). The prediction accuracy was also assessed by comparing predicted and observed mean values for health states valued in the study, using the intraclass correlation coefficient (ICC), the mean absolute error (MAE), and the mean squared error (MSE). Lower MAE and MSE and higher ICC values indicated better accuracy.
After the main analysis, five subgroup analyses were conducted based on five key characteristics of patients with T2DM [33, 34]: (1) current use of injectable treatment, (2) number of medications, (3) presence of needle phobia, (4) duration of injectable treatment, and (5) travel frequency. These analyses aimed to report the significance of parameters and compare disutility values within each subgroup and between groups. By incorporating interaction terms between various attribute levels and subgroup variables, we tested for statistically significant differences in coefficients between subgroups.
All statistical analyses were conducted using STATA 16.0, model coefficients were considered statistically significant if P < 0.05.
Comments (0)