Study design and population
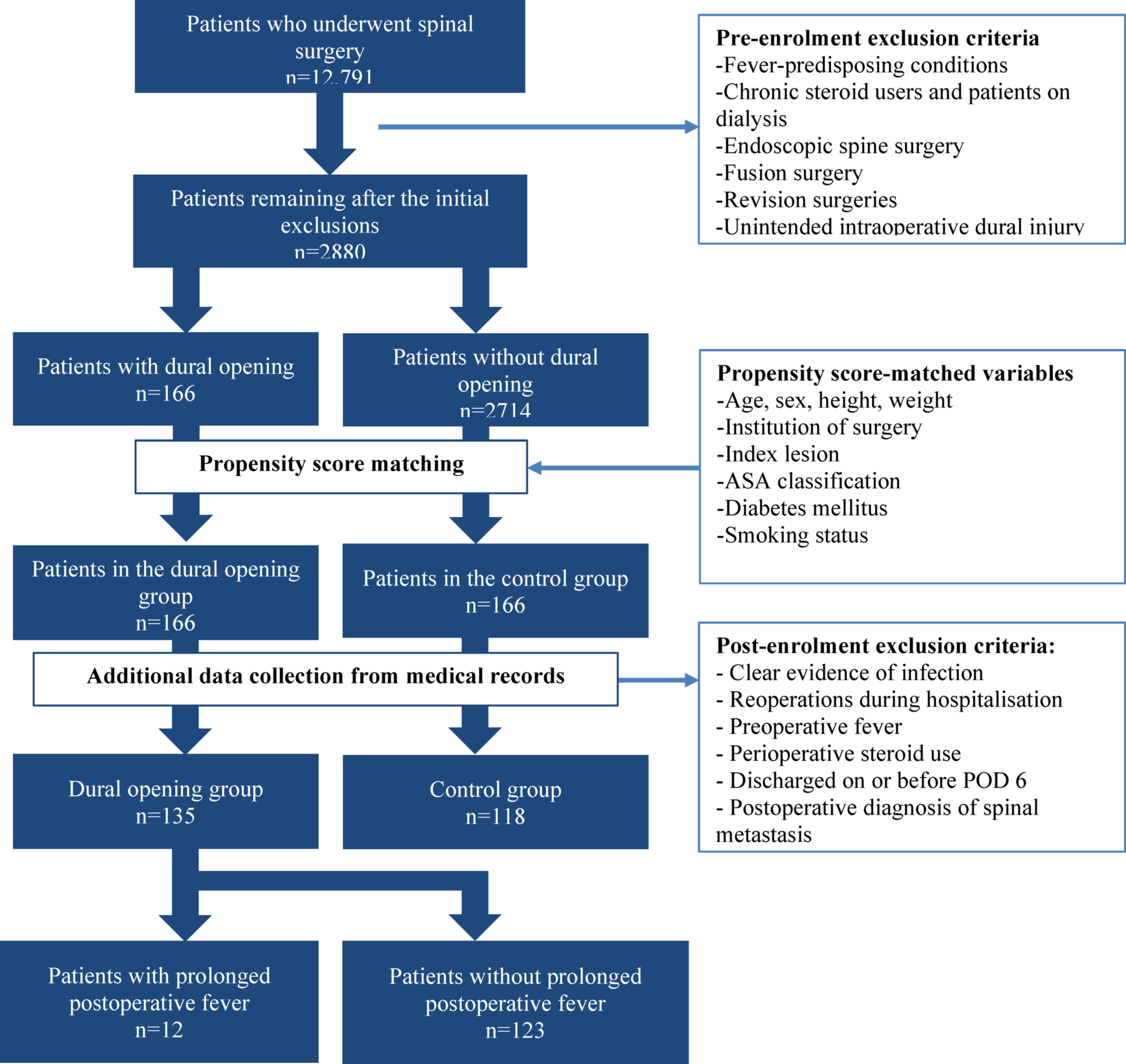
This retrospective multicentre study analysed data from institutional databases at four centres between April 2017 and March 2024. The study included patients who underwent spinal surgery under general anaesthesia. Patients who met the predefined exclusion criteria on the pre-enrolment screening were excluded. The dural opening group included patients who underwent intentional intraoperative dural opening, defined as a planned durotomy to access intradural pathology. From the remaining eligible patients, a control group (non-dural opening group) was selected using propensity score matching (PSM), yielding two comparable cohorts: a dural opening group and a control group.
After applying post-enrolment exclusion criteria, data from both groups were retrospectively analysed for baseline characteristics and postoperative outcomes. Furthermore, a subgroup analysis within the dural opening group compared patients with and without postoperative fever.
Pre-enrolment exclusion criteria
Pre-enrolment exclusion criteria were applied during database screening to minimise confounding from differences in baseline infection risks or surgical invasiveness. Patients were excluded if they were receiving chronic systemic steroids or had dialysis dependence, endoscopic spine surgery, fusion surgery, or revision surgery (including hematoma-induced paralysis, implant failure, hardware removal, or wound dehiscence). Additional exclusions included conditions predisposing to fever (e.g., trauma, active infection, connective tissue disease), unintended intraoperative dural injury to avoid unmeasured heterogeneity in dural-defect size, closure technique (suture, patch, or both), and associated inflammatory response, which could confound comparisons with planned durotomy.
PSM
PSM was performed to balance baseline characteristics between groups. The following variables were selected according to previous reports on risk factors for noninfectious postoperative fever [1,2,3]: age, sex, height, weight, surgical institution, index lesion (cervical/thoracic/lumbosacral), American Society of Anesthesiologists (ASA) class, diabetes mellitus (DM), and smoking history.
Primary outcome and definition
The primary outcome was prolonged postoperative fever, defined as a body temperature ≥ 37.7 °C occurring on or after postoperative day (POD) 7, based on prior reports indicating increased incidences of noninfectious postoperative fever, aseptic meningitis, and reoperations beyond these thresholds [3, 7]. Infectious fever was defined as fever accompanied by clinical symptoms or signs suggestive of infection, combined with at least one of the following criteria: positive microbial culture results, abnormal laboratory findings not attributable solely to surgical stress, or imaging findings consistent with infection. These diagnostic criteria were based on established standards in the previous literature [3]. The day of surgery was designated as POD 0, with postoperative hospital stay calculated such that discharge on POD 0 indicated a 0-day stay, whereas discharge on POD 1 indicated a 1-day stay.
Data collection
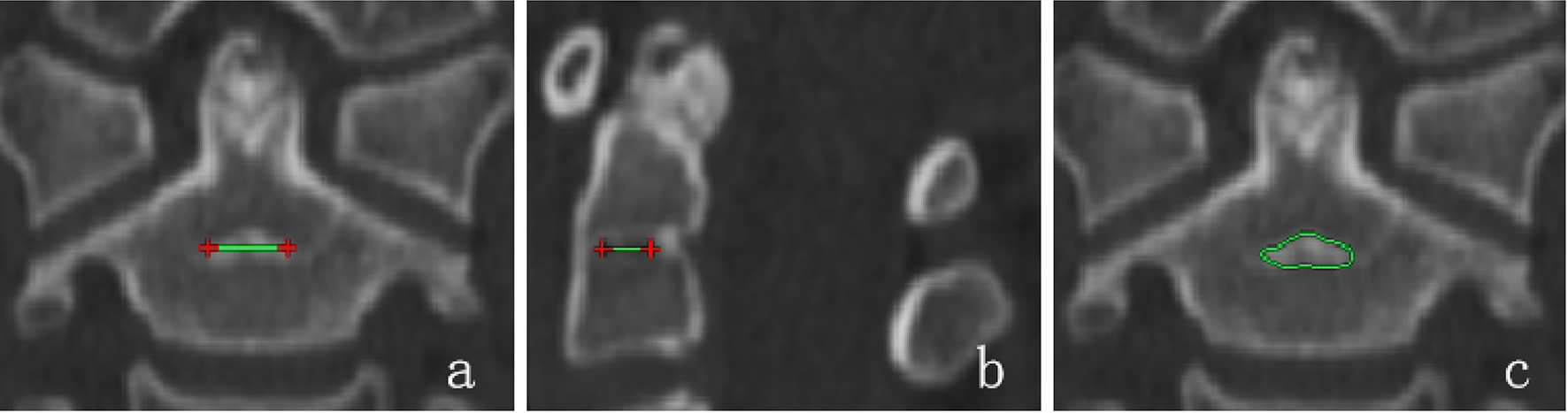
Prespecified variables were extracted from medical records. Physical findings included peak temperature, cumulative fever days, and presence of cerebrospinal fluid (CSF) leakage, defined a priori as low-pressure symptoms with CSF-positive drainage and/or CSF accumulation on MRI. Laboratory data included peak white blood cell (WBC) count, C-reactive protein (CRP) levels, culture results, and tumour pathology; imaging findings included tumour diameters on MRI. Operative characteristics included the cranial-most surgical level (the uppermost level at which the index lesion was addressed), number of decompressed levels, operative time, blood loss, and use of artificial dura for reconstruction. Perioperative management variables included transfusion.
Post-enrolment exclusion criteria
Post-enrolment exclusion criteria were applied after medical record review to minimise confounding and outcome misclassification. Cases were excluded if patients had preoperative fever on the day before surgery; perioperative infection (e.g., surgical-site infection, urinary tract infection, or pneumonia); reoperation during the index hospitalisation; postoperative identification of metastatic cancer; and perioperative steroid exposure (nerve-root or caudal epidural steroid injection, or systemic administration), which possibly modify fever. To ensure adequate observation for the primary outcome (prolonged postoperative fever), patients discharged on or before POD 6 were also excluded.
Statistical analysis
Statistical analyses were performed using JMP Pro version 18.0.1 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at p < 0.05. Categorical variables were analysed using Fisher’s exact test, whereas continuous variables, depending on variance homogeneity, were assessed using unpaired t-tests or Welch’s t-test. For ordinal variables, the Cochran–Armitage trend test was used. We used 1:1 nearest-neighbour PSM (0.2-SD calliper on the logit, without replacement) to reduce confounding and create comparable groups. As a sensitivity analysis, statistical comparisons were performed without applying the post-enrolment exclusions to assess the robustness of the primary findings.

Comments (0)