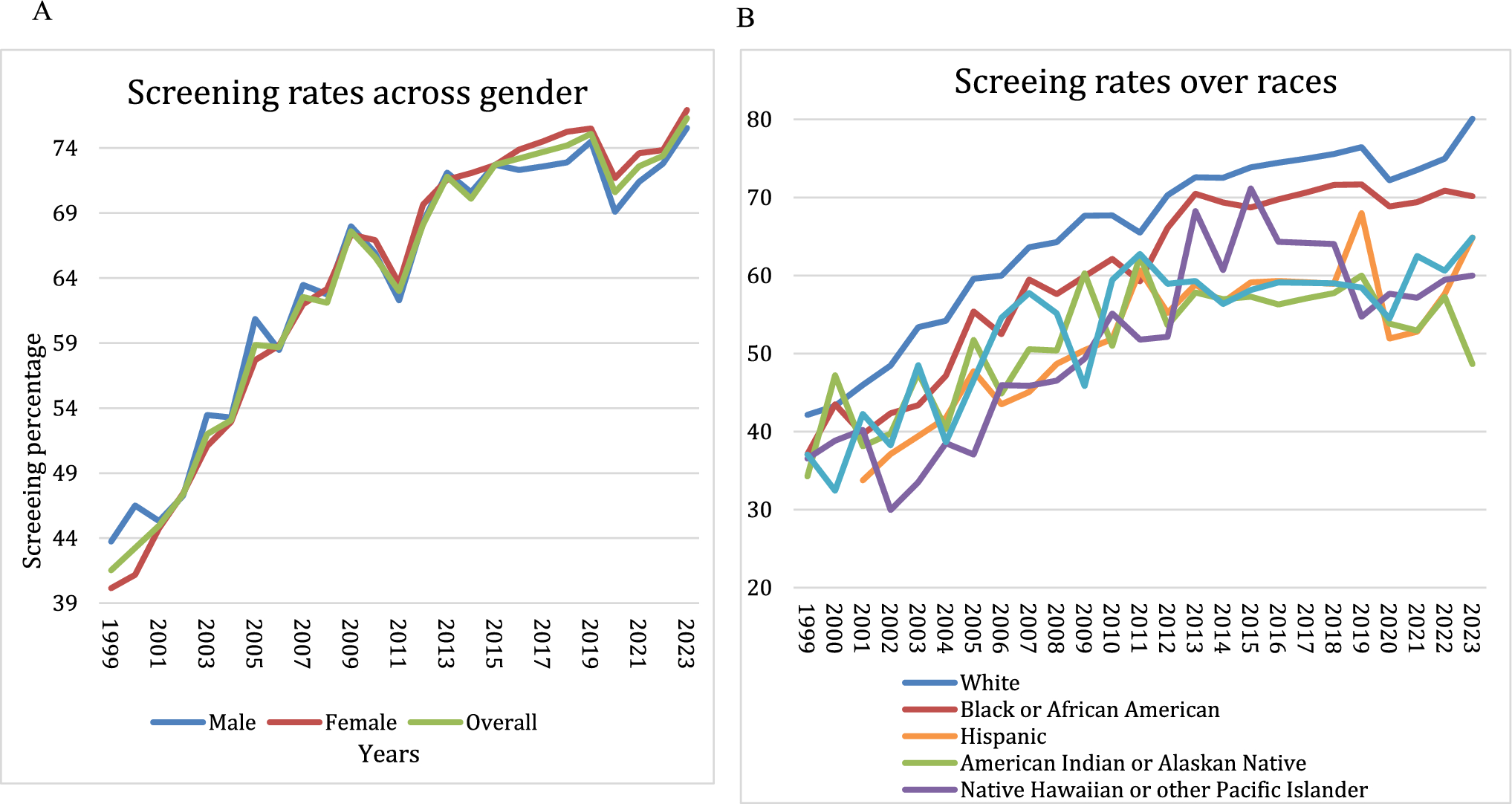
CRC screening is a grade A recommendation from the U.S. Preventive Task Force; this means that with high certainty, screening for CRC in adults between 45 and 75 years has substantial net benefit [12, 13]. The most recent data as of 2021 showed the screening rate among adults between 50 and 75 is 69.9%, which represents an increase from 47.7 in 2005 [14, 15]. While this demonstrates substantial progress over the past two decades, the rate remains below the national target of 80% [16]. In this study, we shed light on the CRC screening rate, mortality, and the projected AAMR at 100% screening rates. Joinpoint analysis revealed multiple changes of the CRC screening throughout the study period. Screening rates increased rapidly during 1999–2006 (APC + 5.50%), rose more modestly in 2006–2013 (APC + 2.41%), and was essentially flat in 2013–2019 (APC + 1.23%). During the COVID period, screening declined in 2019–2021 (APC –2.40%) and rebounded in 2021–2023 (APC + 5.93%).
Overall screening increased from 41.53 to 76.3% between 1999 and 2023, but disparities persisted [17, 18]. These disparities can be explained by barriers, such as socioeconomic status, lack of insurance, and limited education. The increase was most significant between the years 1999 and 2013. The observed increased rates of screening are related to the observed decline in CRC mortality rates. AI/PI, despite their lower screening rates, recorded the lowest overall AAMR. This finding does not align with the traditional models associating lower screening rates with higher mortality. Potential protective factors, such as cultural attitudes toward health and family support systems, may contribute to this discrepancy [19, 20].
When projected at 100% screening rates, the estimated AAMR falls to 18.92 compared to 40.4 per 100,000 in 2023 at a screening rate of 76.30%. However, there is still disparity persisted across races and genders [21, 22]. Also, at 100% screening rates, AA would still show higher mortality rates. This indicates the potential existence of other factors that affect the outcomes. The disparity could be attributed to the fact that they are more likely to present late with advanced disease, increasing mortality even with high screening rates, in addition to the systemic healthcare inequities including delays in diagnosis and treatment as highlighted by other studies [23,24,25].
Although our results are U.S. based, the forces driving screening plateaus and widening disparities are not uniquely to the USA and could reasonably emerge worldwide. Across different health systems, similar barriers limit CRC screening uptake. It is well known that disparities exist between races and different socioeconomic backgrounds [26, 27], similar results were observed, where lower income, lack of insurance, and limited education affected screening rates, compounded by geographic disparities, with rural populations representing additional challenges to healthcare access. Additional barriers common internationally include competing time demands, out of pocket, and indirect costs such as transportation and time off work, low health literacy, cultural and language barriers, and digital access gaps [28,29,30,31,32]. System-level constraints such as long waits for diagnostic colonoscopy after a positive FIT, shortages of trained staff, and limited endoscopy capacity can also limit the effectiveness of screening programs [33, 34]. These challenges were exacerbated by COVID-19 disruptions including temporary program pauses, staff redeployment, and patient hesitancy which were widespread and have left lingering effects on screening recovery worldwide [7, 34]. These barriers will require comprehensive strategies, including community-based programs that provide culturally relevant education and navigation services [35]. Patient education remains the cornerstone in CRC screening. Integrating culturally tailored education and outreach activities recommended by the National Cancer Institute remains a top priority [36]. Furthermore, structured community-based strategies aiming to address barriers faced by minorities and underserved populations, as they are the most vulnerable group, would be beneficial in achieving equity as highlighted by previous research [37, 38]. Implementing electronic physician reminders showed that it is beneficial to increase rates of CRC screening referrals during office visits [39]. Also, involving nonphysician team members has been shown to increase referral rates as it addresses the issue of physicians’ lack of time [40].
Colorectal cancer screening rates showed upward trends until the 2020 COVID pandemic. Then, all cancer screening rates dramatically declined [41]. An international study estimated a global decline of 90%, leading to a 32% reduction in new CRC diagnoses and hence a 53% decline in CRC-related surgeries [42]. Similarly, the study observed a noticeable decline in CRC screening rates in 2020, followed by a gradual increase in subsequent years. Interestingly, the study showed that the disparities in CRC screening increased even more during COVID. The decline in cancer screening rates could be attributed to several reasons, one of them being the temporary closure of screening facilities, with staff shortages and resource relocation toward COVID management [43]. Other population-related causes include patient hesitancy due to fear of contracting the virus, along with the socioeconomic challenges of losing jobs and health insurance [44]. Although COVID is no longer a pandemic, the screening rates did not return to pre-COVID levels. Also, a microsimulation study projected that the pandemic could lead to long-term negative outcomes in CRC indices and mortality [45, 46]. This is a high alarm that we should relocate more resources toward CRC screening advocacy among the population.
The study offered several notable strengths, as it is the first study of its type to involve 25 years, providing a robust longitudinal perspective on CRC screening and mortality rates, taking into consideration the differences among races, genders, socioeconomic standards, and education levels, allowing for comparison and revealing disparities in screening rates and the outcomes. Moreover, this study is unique in the use of projection models in estimating the AAMR at 100% screening rates among the entire population and providing the estimate among minorities and different groups. There are several limitations that affected the study. The use of the BRFSS database comes with the downside that most of the data is self-reported, relying on the accuracy of respondents’ recall ability and truthfulness regarding the screening test and its timing, which can lead to recall bias or reporting bias when individuals do not respond to the survey. Another limitation is that the National Health Interview Survey (NHIS) data does not differentiate between screening and diagnostic colonoscopy and sigmoidoscopy, which, in theory, could create discrepancies between the reported data and real-life data. However, studies have found moderate to good agreement between self-reported data and information from medical records [8]. Additionally, the nature of the CDC WONDER database, which relies on death certificates, may be subject to human error, misidentification of the cause of death, or data loss during file compilation, potentially resulting in underreporting of CRC-related mortality. The database may also lack important individual variables that could influence outcomes, such as healthcare access, comorbidity burden, or medical treatment. Finally, our projection of CRC mortality at 100% screening coverage should be interpreted cautiously. A simple linear association between screening coverage and mortality is unlikely at high coverage levels, because the biologic characteristics of the cancer set limits on what screening can achieve, and some tumors will still escape detection or prevention even under perfect adherence. In addition, there will be many individuals who remain facing structural barriers to CRC screening. Comorbidities including obesity and metabolic conditions, lifestyle behaviors (e.g., smoking, physical activity), will still add to the CRC risk. Moreover, shifts over time in risk factors, improvements in treatment, and changes in stage at diagnosis, along with possible delays between screening uptake and mortality outcomes, may confound the observed relationship. Therefore, the 100% projection is best understood as a scenario-based estimate of possible upper limits, not as a causal prediction.

Comments (0)