Chemotherapy in cancer patients can be associated with the development of cardiomyopathy, which is characterized by a decline in left ventricular (LV) function, leading to symptoms of heart failure (HF) [1]. The incidence of chemotherapy-induced cardiomyopathy (CHIC) has been reported to range from 5 to 10% [2]. However, this rate varies according to patient risk profile, chemotherapy agent, and cumulative dose. CHIC is more frequently seen in elderly individuals, those with multiple comorbidities, or patients with pre-existing cardiovascular disease, as highlighted in the 2022 ESC cardio oncology guidelines [1]. Anthracyclines are the chemotherapy agents most frequently associated with the development of dose-dependent cardiotoxicity and HF [3, 4]. Trastuzumab, a humanized anti-ErbB2 monoclonal antibody, is also associated with a significant incidence of cardiotoxicity, with an increasing risk when used in combination with anthracyclines [5]. The mechanisms underlying the development of CHIC are not fully understood and seem to involve accelerated apoptosis, mitochondrial dysfunction, and impairment in intracellular calcium handling [6]. LV dyssynchrony may also be a manifestation of chemotherapy-induced cardiotoxicity [7].
In addition to optimal medical HF therapy, cardiac resynchronization therapy (CRT) may be a valuable therapeutic option in patients with CHIC with wide QRS duration and LV ejection fraction (LVEF) ≤ 35% [8, 9]. However, CRT appears to be underutilized in cancer patients with HF [9], potentially due to concerns about limited life expectancy, interference with ongoing or planned oncologic treatments, and elevated procedural risks. These risks are particularly relevant in a clinically fragile population and may be further amplified in patients who are immunocompromised. In such cases, immunosuppression can increase susceptibility to device-related complications, including infections, impaired wound healing, and bleeding, especially in the presence of chemotherapy-induced thrombocytopenia or cancer-associated coagulopathies. A careful, multidisciplinary assessment is therefore essential when considering CRT in this setting. Such approach is even more important in this field since outcome measures are limited, and patients with CHIC remain under-represented in CRT trials. Currently available data on CRT efficacy and safety in this population are relatively few and mainly derived from studies with small sample sizes and short-term follow-up. In a systematic review, Shehram et al. showed an improvement in LVEF and NYHA class in patients with CHIC implanted with a CRT device [10]. However, CRT-related effects on LV dyssynchrony, arrhythmic burden, and survival remain only partially explored in this clinical setting.
Aim of this review was to provide a comprehensive update on the effects of CRT in patients with CHIC in terms of LV remodeling, burden of cardiac arrhythmias, and mortality.
Left Ventricular Reverse Remodeling
First, Cardinale et al. described a positive association between LV reverse remodeling achieved with pharmacological therapy and cardiac outcomes in cancer patients with CHIC [2]. In 2008, Ajijola et al. published a case series demonstrating CRT-induced left ventricular reverse remodeling in four patients with CHIC, prolonged QRS duration, and refractory HF despite medical therapy [8]. This study provided the first proof of concept for the benefits of CRT in this patient population.
Main available studies on HF patients with CHIC undergoing CRT are presented in Table 1. The majority of included patients were women, prevalently with a previous history of breast cancer and exposure to anthracyclines. Most patients had left bundle branch block (LBBB) and received a CRT device with defibrillation capabilities. As presented in Table 1, all studies described a CRT-induced improvement in LVEF at follow-up.
Table 1 Main Studies on the Effects of Cardiac Resynchronization Therapy on Left Ventricular Function in Patients with Chemotherapy-induced CardiomyopathyMore in detail, in the retrospective study by Rickard et al. [11], a significant decrease in LV end-diastolic diameter (LVEDD) (− 0.5 ± 0.6 cm, p = 0.013) and LVESD (− 0.7 ± 0.8 cm, p = 0.003) and, accordingly, an increase in LVEF (+ 8.6% ± 9.5%, p = 0.0006) were observed in eighteen patients with doxorubicin-induced cardiomyopathy after CRT over a mean follow-up of 9.1 ± 6.3 months. The positive effects on LV remodeling were associated with an improvement in NYHA functional class from 2.9 ± 0.3 to 2.4 ± 0.3 (p = 0.003). Despite a significantly shorter QRS duration (136 ± 29 ms vs 159 ± 32 ms, p = 0.0073), CRT patients with CHIC showed similar enhancements in echocardiographic and functional variables as compared to CRT patients with other forms of non-ischemic cardiomyopathy. It should be noted that the results may be influenced by the selection criteria for CRT adopted in the study, which also included narrow QRS (< 120 ms) with echocardiographic evidence of mechanical dyssynchrony, criteria no longer supported by current guidelines. In this study, the diagnosis of doxorubicin-induced cardiomyopathy was based solely on clinical history and basic cardiac workup, thereby limiting diagnostic certainty.
Similar results were described in two recent retrospective observational studies by Ezzeddine et al. [12] and Patel et al. [13]. In the former study, 29 cancer patients with CHIC, mostly (90%) treated with doxorubicin, underwent CRT implantation after failing to respond to at least three months of optimal medical therapy [12]. The mean QRS duration was 146 ± 26 ms and 55% of patients had a LBBB morphology. At 6–18 months of follow-up, LVEDD and LVESD decreased from 60 ± 8 mm to 56 ± 8 mm (p = 0.006) and from 52 ± 8 mm to 45 ± 8 mm (p = 0.002), respectively. Meanwhile, LV end-diastolic volume (LVEDV) and LV end-systolic volume decreased from 207 ± 76 ml to 165 ± 53 ml (p = 0.065) and from 148 ± 65 ml to 95 ± 36 ml (p = 0.109), respectively. Accordingly, the LVEF increased from 28% ± 8% to 38% ± 10% (p < 0.001). Although not statistically significant, patients with LBBB showed a trend toward greater improvement in LVEF and LV reverse remodeling. The proportion of patients with a post-CRT decrease in LVESD and LVESD of ≥ 15% was comparable between cancer patients with CHIC and controls (48% vs. 37%, p = 0.3, and 67% vs. 63%, p = 0.8, respectively). The control group consisted of 58 non-cancer patients with other forms of non-ischemic cardiomyopathy. Older age was identified as a predictor of a ≥ 15% decrease in LVESD at follow-up.
Patel et al. [13] performed a retrospective study on 34 cancer patients with a diagnosis of anthracycline-induced cardiomyopathy who underwent CRT implantation after 3 months of ineffective HF therapy. Response to CRT was defined as an improvement in LVEF ≥ 10%, as assessed by echocardiography during follow-up sessions. The mean QRS duration was 139 ± 34 ms and 56% of patients had a LBBB morphology. At 9.6 ± 8.1 months after CRT implantation, LVEF increased from 21.8% ± 7.6% to 30.4% ± 13.0% (p < 0.001) and the NYHA class decreased from 3.1 ± 0.3 to 2.3 ± 0.8 (p = 0.001). According to authors’ definition, 44% of patients were structural responders, exhibiting an improvement in LVEF ≥ 10%. An improvement in LVEF of at least 5% after CRT implantation was found in 63% of patients. Baseline LBBB morphology (odds ratio: 6.29 [1.29–30.54]) and LVEDD (odds ratio: 0.22 [0.06–0.78]) were identified as predictors of CRT response. Consistent with a lower-level recommendation in both the European [14] and American [15] guidelines, only 23% of patients with CHIC and a non-LBBB morphology resulted responders to CRT. A propensity matched analysis using as group of control 369 consecutive patients with other forms of non-ischemic cardiomyopathy, who underwent CRT implantation during the same period, revealed similar improvement in LVEF. It is important to note that no relationship was observed between the time since either malignancy diagnosis (mean: 11.3 years) or last chemotherapy exposure (mean: 10.2 years) and the likelihood of response to CRT. Both studies by Ezzedine et al. [12] and Patel et al. [13] are limited by small sample sizes and the absence of a CHIC control group without CRT, which precludes comparison with medical therapy.
The Multicenter Automatic Defibrillator Implantation Trial-Chemotherapy-Induced Cardiomyopathy (MADIT-CHIC) is the only prospective trial currently available investigating the role of CRT in 30 cancer patients with CHIC [16]. All patients exhibited a LBBB morphology, with a median QRS duration of 152 ms (interquartile range: 142–160 ms). Echocardiographic follow-up, scheduled at 6 months after CRT implantation, showed a decrease in LV volumes (end-systolic −37.0 ± 20.4 ml and end-diastolic −31.9 ± 22.5 ml, both p < 0.001) and an increase in LVEF from 28 to 39% (p < 0.001). Probably because all the patients had LBBB, the relationship between baseline QRS duration and reverse remodeling was weakened. Moreover, a reduction in left atrial volume (from 60.3 ml to 47.9 ml, p < 0.001) was observed. Overall, NYHA class improved in 41% of patients. Finally, although a control group is lacking, the degree of CRT-mediated LV reverse remodeling was comparable to that achieved in HF patients with non-ischemic cardiomyopathy enrolled in the MADIT-CRT (Multicenter Automatic Defibrillator Implantation Trial—Cardiac Resynchronization Therapy) study [17]. Notably, as observed in Patel’s study [13], the lengthy interval (median: 13.8 years) between cancer diagnosis and CRT implantation does not appear to affect the benefit provided by biventricular pacing. The elapsed time between the last anthracycline administration and CRT implantation was not provided by the authors. However, the limited sample size and absence of a control group affect the overall generalization of the results, while the locally adjudicated diagnosis of CHIC by center investigators, and reliance on 2D echocardiography introduce potential bias and measurement limitations.
Left Ventricular Dyssynchrony
The exact mechanisms driving the benefits of CRT in cancer patients with CHIC remain unknown. In the MADIT-CHIC study [16], the authors suggested that CRT exerts its effects by reducing mechanical dyssynchrony associated with LBBB. However, no imaging investigations were conducted to assess mechanical dyssynchrony before and after CRT. Such data could have helped rule out confounders (e.g., optimization of drug dosage) and clarified the true mechanism behind reverse remodeling and LVEF improvement. Therefore, the authors’statement remains purely speculative.
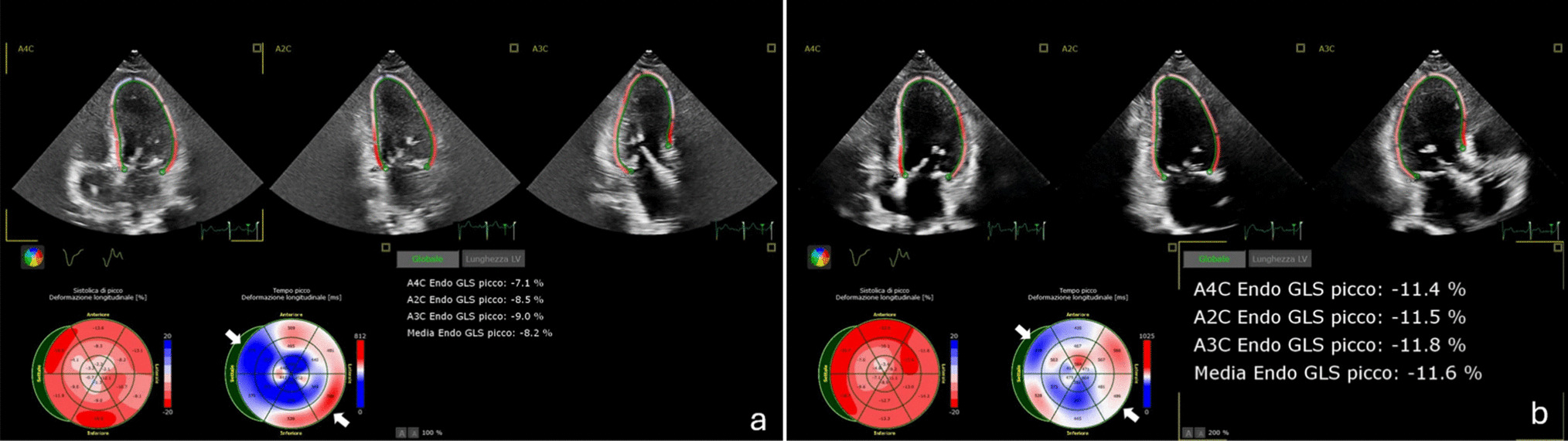
The only CRT study that has provided data on the direct assessment of changes in LV mechanical dyssynchrony in patients with CHIC is that of Ezzeddine et al. [12]. LV global longitudinal strain (GLS), LV systolic strain rate, and LV early diastolic strain rate were evaluated by 2D speckle-tracking strain imaging. Patients with non-ischemic cardiomyopathy, including CHIC, showed improvement in LV GLS after CRT. No difference in the average change in GLS after CRT was observed between patients with CHIC and those with other forms of non-ischemic cardiomyopathy (−2.15 ± 4.32 vs. −3.57 ± 4.02, p = 0.19). Consistently, the average changes in LV systolic and early diastolic strain rates were similar between the two groups.
Mortality
In the retrospective study by Patel et al. [13], after a mean follow-up of 6.9 ± 4.0 years from CRT implantation 56% of patients with anthracycline-induced cardiomyopathy met the endpoint of mortality, LV assist device implantation, or heart transplantation. CRT responders, identified by an improvement in LVEF of at least 10% at follow-up, had better survival rates than non-responders (p = 0.012). In a propensity matched analysis, no significant differences in LVEF improvement and long-term survival rates were found between patients with anthracycline-induced cardiomyopathy and patients with other aetiologies of non-ischemic cardiomyopathy undergoing CRT implantation [13]. These results confirmed previous data suggesting a similar mortality rate between CRT patients with anthracycline-induced cardiomyopathy and other forms of non-ischemic cardiomyopathy over a mean follow-up of 3.1 ± 0.9 years (23.5% vs 17.7%, p = 1.0) [11]. In the study by Rickard et al. [11], it was not possible to discriminate between deaths due to worsening HF or cancer progression. Also, in the retrospective study by Ezzeddine et al. [12], overall mortality was similar between patients with CHIC and patients with other forms of non-ischemic cardiomyopathy (48.2% versus 34%, p = 0.214) at a median follow-up time of 6 years. In the prospective MADIT-CHIC trial [16], no deaths in the 30 enrolled patients were observed at 6-month follow-up.
Cardiac Arrhythmias
In patients with CHIC, structural and hemodynamic changes may lead to electrical instability and induce cardiac arrhythmias [6]. Few data are available on the effects of CRT on cardiac arrhythmias in the setting of CHIC. In a retrospective cohort study evaluating the burden of cardiac arrhythmias in patients with anthracycline-related cardiomyopathy implanted with an ICD or CRT-D device [18], the most common arrhythmia was nonsustained ventricular tachycardia, followed by atrial fibrillation, sustained ventricular tachycardia or ventricular fibrillation. The incidence and type of arrhythmia, as well as device interventions, were similar in patients with anthracycline-related cardiomyopathy compared to cancer patients with non-anthracycline-related cardiomyopathy and non-cancer patients with ischemic heart disease or dilated cardiomyopathy. The 5-year rate of ICD therapies was 19.9% in patients with anthracycline-related cardiomyopathy compared to 22.1% in cancer patients with non-anthracycline-related cardiomyopathy (p = 0.93) and 32.6% in patients with ischemic-related LV dysfunction or non-ischemic dilated cardiomyopathy (p = 0.14, for both). Overall survival of patients with anthracycline-related cardiomyopathy was similar to the other groups.
Given the significant arrhythmic risk combined with the clinical frailty of CHIC patients, remote monitoring and wearable cardiac technologies may enable timely arrhythmia detection, facilitate prompt clinical interventions, and support more flexible telemedicine-based follow-up. Moreover, these technologies may reduce the need for frequent hospital visits, thereby alleviating the social and logistical burdens faced by this vulnerable patient population.
Optimizing the timing of CRT implantation
Similar to other non-ischemic cardiomyopathies caused by cardiotoxic agents (e.g., alcohol), CHIC is often reversible, with a higher likelihood of LV reverse remodeling and LVEF recovery following chemotherapy withdrawal and optimized medical therapy. This potential for recovery should guide the timing of CRT implantation, to avoid unnecessary procedures that carry costs and device related risks. Therefore, timing of CRT implantation in patients with CHIC must be carefully individualized and should account not only for conventional electrophysiological and functional criteria, but also for oncologic status (e.g., active disease vs remission), estimated non-cardiac prognosis, and potential need for thoracic radiotherapy.
Although studies such as MADIT-CHIC [16] and the one by Rickard et al. [11] demonstrated significant improvements in LVEF and LV remodeling after CRT implantation in patients with persistent dysfunction, they did not explicitly use estimated survival as an inclusion criterion. However, it is clinically reasonable to consider CRT primarily in patients in cancer remission with an expected survival greater than 12 months, to ensure sufficient time to derive meaningful benefit from device therapy. This consideration is particularly relevant because the effects of CRT on ventricular remodeling are time-dependent, and the maximum benefit is typically observed between 3 and 9 months after implantation. Furthermore, reductions in ventricular volumes achieved during this period have been shown to be sustained for up to 3 years, with this effect being more pronounced in patients with non-ischemic cardiomyopathy [19]. Therefore, adequate life expectancy is essential to allow patients to experience the full benefits of CRT.
Moreover, data from Ezzedine et al. [12] and Patel et al. [13] support a strategy of allowing a period of at least 3 months of optimal medical therapy before considering CRT implantation. In both studies, patients underwent CRT only if LV dysfunction was persistent despite current guideline-directed therapy, reinforcing the importance of a structured evaluation period to differentiate between reversible cardiotoxicity and stable LV impairment.
Conversely, in patients with active malignancy or limited life expectancy, CRT might be considered only when symptomatic burden is high, in an attempt to improve quality of life, provided that device implantation does not interfere with ongoing cancer treatments. In particular, in cases where thoracic radiotherapy is expected, the risks of lead fibrosis, device malfunction, or interference with cancer therapy must be weighed against CRT potential cardiac benefit [20].
In this context, the multidisciplinary team plays a pivotal role. An integrated cardio-oncological approach is essential for early identification of patients susceptible to recover ventricular function with medical therapy alone after cessation of cardiotoxic regimens, based on baseline cardiovascular risk and early signs of subclinical myocardial impairment assessed through cardiovascular imaging and biomarkers surveillance. Advanced imaging techniques and novel biomarkers are increasingly valuable in stratifying the likelihood of cardiac function recovery in CHIC patients [21]. Cardiac magnetic resonance, particularly tissue characterization through T1 mapping and extracellular volume assessment, can help identify patients less likely to experience LV reverse remodeling following medical therapy, especially those with persistent and diffuse fibrosis or myocardial edema [22]. Similarly, elevated levels of a soluble form of suppression of tumorigenicity 2 (> 48 ng/mL) have been associated with poor reverse remodeling, likely reflecting fibrotic burden [23]. In such high-risk patients, timely referral for CRT evaluation (possibly with defibrillator backup) may improve outcomes and, thus, may be justified. In contrast, in patients with reversible myocardial injury and favorable prognostic indicators, based on the absence of fibrosis and favorable biomarker profiles, a more conservative approach may be adopted, avoiding premature device implantation. Additionally, early changes in traditional biomarkers such as NT-proBNP may offer rapid insights into LV reverse remodeling dynamics. In the PROVE-HF study, NT-proBNP levels began to decline within 2 weeks of initiating sacubitril/valsartan, anticipating structural improvements seen at 6 months [24]. In these patients, a period of monitoring and optimization of HF guideline-directed medical therapy may allow recovery.
Structured cardio-oncology programs that incorporate standardized surveillance protocols and early referral pathways have been shown to improve cardiovascular outcomes and facilitate timely CRT evaluation when indicated [25]. Close collaboration between oncologists, cardiologists, and electrophysiologists is therefore critical to ensure appropriate selection and optimal timing of CRT in this complex and heterogeneous population. Clinical, social, and health-care issues should be taken into consideration in the management of CHIC patients.

Comments (0)