
Remember me
Cancer therapy has significantly improved survival in oncology patients [1]; however, the associated cardiotoxicity remains a major concern, which negatively affects both quality of life and prognosis [2]. The risk of cardiac damage is not the same for all cancer patients, depending on their cardiovascular (CV) profile combined with therapy-related factors, such as drug type and dosage. Early detection and management of therapy-induced cardiotoxicity are essential to mitigate CV complications without compromising treatment efficacy [3]. Echocardiographic evaluation plays a key role in this context, providing a non-invasive and reliable method to monitor cardiac function and detect subclinical dysfunction. In this regard, speckle-tracking derived global longitudinal strain (GLS) has emerged as a highly sensitive marker for identifying early myocardial damage since its impairment often precedes a decline in left ventricular ejection fraction (LVEF) [4, 5]. Effective management of cardiac involvement requires a multidisciplinary approach. Collaboration between cardiologists and oncologists is essential to ensure optimal therapeutic outcomes, balancing cancer treatment efficacy with CV safety [6]. The aim of the present review is to provide both cardiologists and oncologists with a practical tool that can be useful in writing and interpreting echocardiographic reports, respectively. To achieve this goal, key aspects of cardiac systolic and diastolic function, pericardial disease, valvular heart disease, intracardiac masses, and their prognostic value in the field of cardio-oncology are discussed. Moreover, a therapeutic algorithm is proposed, focused on both cancer treatment management and cardioprotective strategies in selected contexts. This guidance may help bridge the gap between the two specialties by providing oncologists with essential insights to effectively integrate CV assessments into their therapeutic decision-making process.
Cardiotoxicity risk stratification: identification of cancer patients requiring baseline echocardiographyBaseline cardiotoxicity risk stratification represents a crucial step before initiating cancer therapy, as it guides both the appropriate use and optimal timing of echocardiographic evaluation. However, assessing cardiotoxicity risk can be challenging due to multiple confounding factors, including the concomitant use of agents with adverse metabolic effects (e.g., corticosteroids). The 2022 European Society of Cardiology (ESC) guidelines on cardio-oncology [6] support the use of the recently developed Heart Failure Association (HFA) and International Cardio-Oncology Society (IC-OS) baseline risk stratification tool. According to this tool, cardiotoxicity risk is based on the patient’s specific cancer therapy and underlying CV profile (Table S1, Supplementary Material) [7]. Transthoracic echocardiography (TTE) at baseline is recommended for patients with a high or very high CV risk profile or for those receiving cardiotoxic cancer therapies [8]. Individuals with significant valvular heart disease, history of myocardial infarction, prior coronary revascularization, or stable angina, as well as those with baseline LVEF < 50% or age ≥ 80 years, and individuals with pre-existing heart failure or cardiomyopathy are considered respectively at high and very high risk for cardiotoxicity prior to starting anthracycline or human epidermal growth factor receptor 2 (HER2)-targeted therapies. Different classes of cancer therapy are possibly associated with distinct cardiotoxic findings detectable on TTE (Table 1) [2, 9,10,11,12,13,14,15,16,17,18,19,20]. It should be underlined that CV risk stratification does not aim to exclude high and very high-risk patients from cancer treatment, but to ensure that patients from all risk categories receive the best possible treatment. There is often a tendency to underestimate and undertreat CV risk factors in cancer patients [21]. However, the presence of untreated CV risk factors may potentiate oncology drugs’ cardiac toxicity [22, 23]. Therefore, reducing cancer patients’ CV risk is crucial for them to tolerate cardiotoxic treatments more easily.
Table 1. Echocardiographic findings associated with different classes of cancer therapiesChemotherapy-related left heart dysfunction: key echocardiographic parameters and their interpretationCancer therapy can adversely affect cardiac structure and function, leading to either asymptomatic cardiac dysfunction or symptomatic heart failure (HF). This condition is collectively termed cancer therapy-related cardiac dysfunction (CTRCD). The most recent definition of CTRCD, derived from the 2022 IC-OS consensus statement [24], is based on changes in LVEF, systolic dysfunction, and/or HF events. LVEF assessed by biplane Simpson’s method remains the most commonly used parameter for the identification of left ventricular (LV) dysfunction before, during, and after cancer therapy. However, it is important to acknowledge the inherent limitations of LVEF measurement, including intra- and inter-operator variability [25] and hemodynamic load-dependence. When available, three-dimensional (3D) echocardiography should be preferred for LVEF assessment, as it provides greater accuracy and reproducibility [25]. However, its feasibility may be reduced in conditions that limit the acoustic window and the quality of ultrasound imaging [26]. It is the case for cancer patients who undergo concomitant radiotherapy (e.g., for breast cancer or lymphoma) and surgical interventions (e.g., mastectomy, breast implants/expanders). When image quality is suboptimal, the use of ultrasound contrast agents enhances the delineation of the endocardial border, improving the assessment of LVEF and LV volumes [27]. In contemporary cardiology, GLS has emerged as an earlier, more sensitive, and more reproducible marker of myocardial dysfunction than LVEF [4, 5], with strong evidence supporting its diagnostic and prognostic value also in cancer patients [28, 29]. A relative change in GLS has been proposed as an optimal parameter for detecting asymptomatic mild CTRCD [24, 30, 31]. Various threshold values have been explored over the last few years [32, 33]. Currently, a relative GLS reduction greater than 15% from baseline is the recommended threshold for the diagnosis of CTRCD, as this value seems to predict future significant decline in LVEF [29]. GLS measurements obtained by using 3D speckle-tracking echocardiography proved to have added value over two-dimensional (2D) speckle-tracking echocardiography in detecting cardiotoxicity [34]; however, its routine clinical use remains limited due to some critical constraints, including the need for optimal acoustic windows and high-quality images, specialized training, and the lack of standardization across vendors. LV myocardial work indices (MWIs), obtained from speckle-tracking derived strain parameters and non-invasive measured systolic blood pressure, have shown potential in improving the diagnosis and prognosis of CTRCD. A reduction in the global work index, particularly in patients with only a minor reduction in GLS but a significant decline in systolic blood pressure (~ 21 mmHg), may help identify patients at higher risk of CTRCD [35]. However, the optimal thresholds for the sequential use of GLS and MWIs require validation through large multicenter studies before clinical implementation.
The 2022 ESC guidelines on cardio-oncology [6] do not explicitly include LV diastolic dysfunction among the echocardiographic abnormalities for the diagnosis of CTRCD. Also, they do not provide specific recommendations on using diastolic dysfunction for initiating cardioprotective therapy or discontinuing cancer treatment. Nevertheless, evidence suggests that traditional indices of diastolic function [36] can also change during cancer treatment and could serve as early markers of subsequent systolic dysfunction, particularly in patients receiving anthracyclines and/or trastuzumab [31, 37, 38].
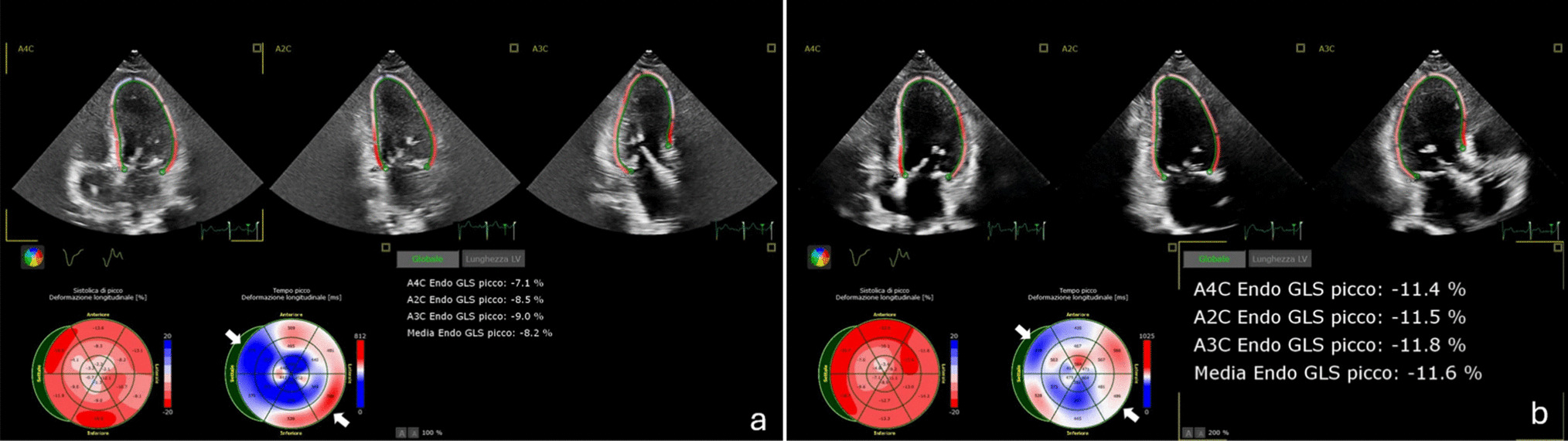
While the role of LV GLS in cardio-oncology is well characterized, little is known about the role of left atrial (LA) strain, which has been recently identified as a potential indicator of subclinical or early diastolic dysfunction [39, 40]. The STRANO study evaluated LA function using speckle-tracking echocardiography in women receiving chemotherapy for breast cancer. The results showed that LA strain impairment was significantly greater in patients who developed asymptomatic mild CTRCD [41]. Therefore, LA strain may serve as a promising parameter in this setting, warranting further validation. The prognostic significance and clinical utility of diastolic dysfunction remain poorly defined, highlighting the need for further research to clarify its relevance and potential implications in cardio-oncology. In Table 2. a checklist of the key echocardiographic parameters that should not be missing from an oncology patient’s report and their practical interpretation are reported. Complementary echocardiographic acquisitions are shown in Figure 1.
Fig. 1
Key echocardiographic acquisitions during oncology patient’s evaluation. 1 Left ventricular systolic functionassessment by traditional Simpson biplane method (1A) and speckle tracking-derived global longitudinal strain (1B). 2Left ventricular diastolic function assessment by traditional methods (E/e′ ratio in 2 A) and left atrial strain (2B). 3 Aorticregurgitation (3A) and mitral regurgitation (3B) in patients undergone chest radiotherapy. 4 Right ventricular systolicfunction assessment by traditional methods (TAPSE and S′ wave velocity in 4 A) and speckle tracking echocardiography(4B). 5 Echocardiographic signs of pulmonary embolism in a cancer patient. 6 Pericardial effusion in a cancer patient
The decision to initiate cardioprotective treatment or discontinue cancer therapy should be based on a comprehensive evaluation of multiple factors, including the severity of both cancer and CV symptoms, cancer prognosis, the availability of alternative cancer treatments, potential adverse drug reactions and interactions, and the patient’s preferences. A comprehensive and flexible diagnostic and therapeutic algorithm for the management of CTRCD, based on the integration of current guidelines and clinical experience, and potentially applicable across all classes of oncologic treatments, is proposed in Fig. 2. This flowchart integrates the different severity grades of CTRCD, including isolated diastolic dysfunction, and offers guidance on whether to continue or interrupt cancer treatment, as well as when to initiate cardioprotective therapy.
Fig. 2
Diagnostic and therapeutic algorithm for the management of cardiac dysfunction induced by cancer therapy. ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin II receptor blockers; CTRCD, cancer therapy-related cardiac dysfunction; CTR-RVT, cancer therapy-related right ventricular toxicity; FAC, fractional area change; GLS, global longitudinal strain; HF, heart failure; LA, left atrium; LAVi, left atrial volume index; LVEF, left ventricular ejection fraction; PAH, pulmonary arterial hypertension; PE, pulmonary embolism; RV, right ventricle; RV-FWS, right ventricular free wall strain; SGLT2, sodium–glucose cotransporter 2; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation
Table 2 Checklist of the key parameters to include in the echocardiographic report of oncology patients and their clinical implicationsRight heart evaluation in patients undergoing cancer therapy: essential information for practiceHistorically, studies on cancer-related toxicity have focused on the assessment of LV dysfunction. However, the impact of oncologic therapy on the right ventricle is increasingly recognized and has become the subject of growing clinical and scientific interest [42, 43]. A recent scientific statement by the HFA of the ESC and the ESC Council of Cardio-Oncology has proposed a new classification of cancer therapy-related right ventricular toxicity (CTR-RVT) based on two categories: symptomatic CTR-RVT, defined by right heart morpho-functional abnormalities with clinical signs and symptoms of right ventricular (RV) failure; asymptomatic CTR-RVT, defined as a > 15% reduction from baseline in RV free wall strain (RV-FWS) in the absence of significant impairment in other parameters, including 3D derived RV ejection fraction (Fig. 2) [44].
TTE represents the primary imaging modality for evaluating RV in cancer patients (Table 2, Fig. 1). Current cardio-oncology guidelines emphasize the importance of a baseline morphologic and functional evaluation of the RV in all oncologic patients referred for TTE. This recommendation is particularly relevant for patients with pre-existing conditions or at risk for RV dysfunction or scheduled to receive agents more frequently associated with RV and pulmonary circulation toxicity (e.g., anthracyclines, trastuzumab, cyclophosphamide, or dasatinib) [6, 45]. RV impairment typically develops concomitantly with LV dysfunction but may also occur in isolation [46]. Radiotherapy (RT) may contribute to RV dysfunction through direct cellular injury, amplified by the anatomical anterior position and thinner wall of the RV [42, 44].
The alteration of conventional parameters of RV systolic function during chemo-radiotherapy, including tricuspid annular plane systolic excursion (TAPSE), tricuspid annulus systolic velocity (S’ wave) obtained by tissue Doppler imaging, and fractional area change, is indicative of overt dysfunction, providing limited sensitivity for the early impairment [44]. Several studies showed a consistent decline in RV longitudinal strain parameters associated with cancer therapy, with more robust data about RV-FWS [47,48,49]. This impairment in the context of anthracycline-induced toxicity appears to exhibit a dose-dependent pattern [50]. Importantly, RV longitudinal strain values may decline during the early phase of CTR-RVT, when traditional echocardiographic parameters remain normal, being a valuable marker for subclinical dysfunction [42, 44]. In a cohort of 128 patients diagnosed with non-small cell lung cancer undergoing chemo-radiotherapy, significant alterations in both RV-GLS and RV-FWS were observed, despite no significant changes being observed in other conventional measures. Notably, RV-FWS demonstrated a correlation with 6-month all-cause mortality, underscoring its potential value as a prognostic marker [42]. Emerging evidence suggests that 3D strain may offer greater sensitivity for detecting RV subclinical dysfunction [46, 48]. Nonetheless, its routine application remains limited by the availability of specific software and technical challenges.
When feasible, 3D RV ejection fraction (RVEF) also provides incremental prognostic value over traditional 2D RV systolic function parameters [51] in patients undergoing cancer therapy. In a population treated with anthracyclines, Shen et al. [52] demonstrated that a 3D RVEF reduction was associated with worse outcomes, particularly when combined with an impaired LV GLS. However, similarly to conventional 2D parameters, a decrease in 3D RVEF may solely reflect a later stage of RV dysfunction.
As part of the right heart evaluation, it is important to routinely look for signs of RV acute and chronic overload. Pulmonary embolism (PE) is frequent in cancer patients due to several factors, such as the hypercoagulable state, surgical interventions, chemotherapy, and the use of central venous catheters [53]. TTE has limited negative predictive value in PE diagnosis, and the presence of specific echocardiographic signs, including the widely recognized “McConnell sign,” is relatively uncommon [54, 55]. Rarely, mobile thrombi “in transit” may be visualized in the right heart on TTE or transoesophageal echocardiography (TOE), a finding associated with a high mortality rate [56]. TTE remains a valuable tool for assessing hemodynamic instability secondary to PE and RV dysfunction, which, when present, is associated with worse prognosis [54, 57, 58]. In the context of acute PE, the non-adapted RV is unable to generate elevated pressures in response to an increased afterload; consequently, tricuspid regurgitation velocity (TRV) rarely exceeds 3.4 m/s, generating a tricuspid regurgitation pressure gradient (TRPG) ≤ 45 mmHg. Accordingly, the so-called 60/60 sign—defined as a pulmonary artery acceleration time ≤ 60 ms associated with a TRPG ≤ 60 mmHg—has been described [59].
Pulmonary hypertension (PH) is relatively common in cancer patients due to concomitant cardiopulmonary comorbidities, CTRCD, recurrent subclinical PE, or cancer-related pulmonary microangiopathy [60]. Furthermore, certain cancer treatments may contribute to PH development [44], such as dasatinib, which has been associated with pulmonary arterial hypertension (PAH) [55]. Current European guidelines on cardio-oncology recommend the discontinuation of dasatinib, even in asymptomatic patients, in cases of TRV exceeding 3.4 m/s or in the presence of confirmed PAH on right heart catheterization [6]. Radiation therapy and bleomycin may also lead to interstitial pulmonary fibrosis, potentially involving the pulmonary microvasculature and thereby increasing pulmonary vascular resistance [61]. Alkylating agents, interferon therapy, immune checkpoint inhibitors (ICI), and proteasome inhibitors have also been associated with the development of PH [62]. Moreover, surgical procedures such as lobectomy for lung cancer may result in an increased RV afterload attributable to a diminution of the pulmonary vascular bed [63]. In the case of chronic PH, signs of chronic RV pressure overload (e.g., subcostal RV free wall thickness > 5 mm and an enlarged right atrium in comparison to the left atrium) can be found [64], and TRV > 3.4 m/s (TRPG > 60 mmHg) is more frequently observed [65].
Recent studies have emphasized the prognostic value of arterial ventricular uncoupling, as assessed by the ratio between TAPSE and pulmonary artery systolic pressure (PASP) on echocardiography, in both PE and PH [66, 67]. A TAPSE/PASP ratio < 0.67 has been shown to be independently associated with increased all-cause mortality in patients with non-small cell lung cancer undergoing pulmonary resection [63]. Finally, echocardiography-derived pulmonary artery pulsatility index (PAPI) is emerging as a superior marker compared to TAPSE for predicting mortality in right heart failure conditions, including acute PE and PH [68, 69].
Beyond function: echocardiographic assessment of the pericardium, valves, and cardiac massesPericardial involvement due to direct tumor infiltration, chemo-, or radiotherapy is a relatively frequent finding in cancer patients [70,
Comments (0)