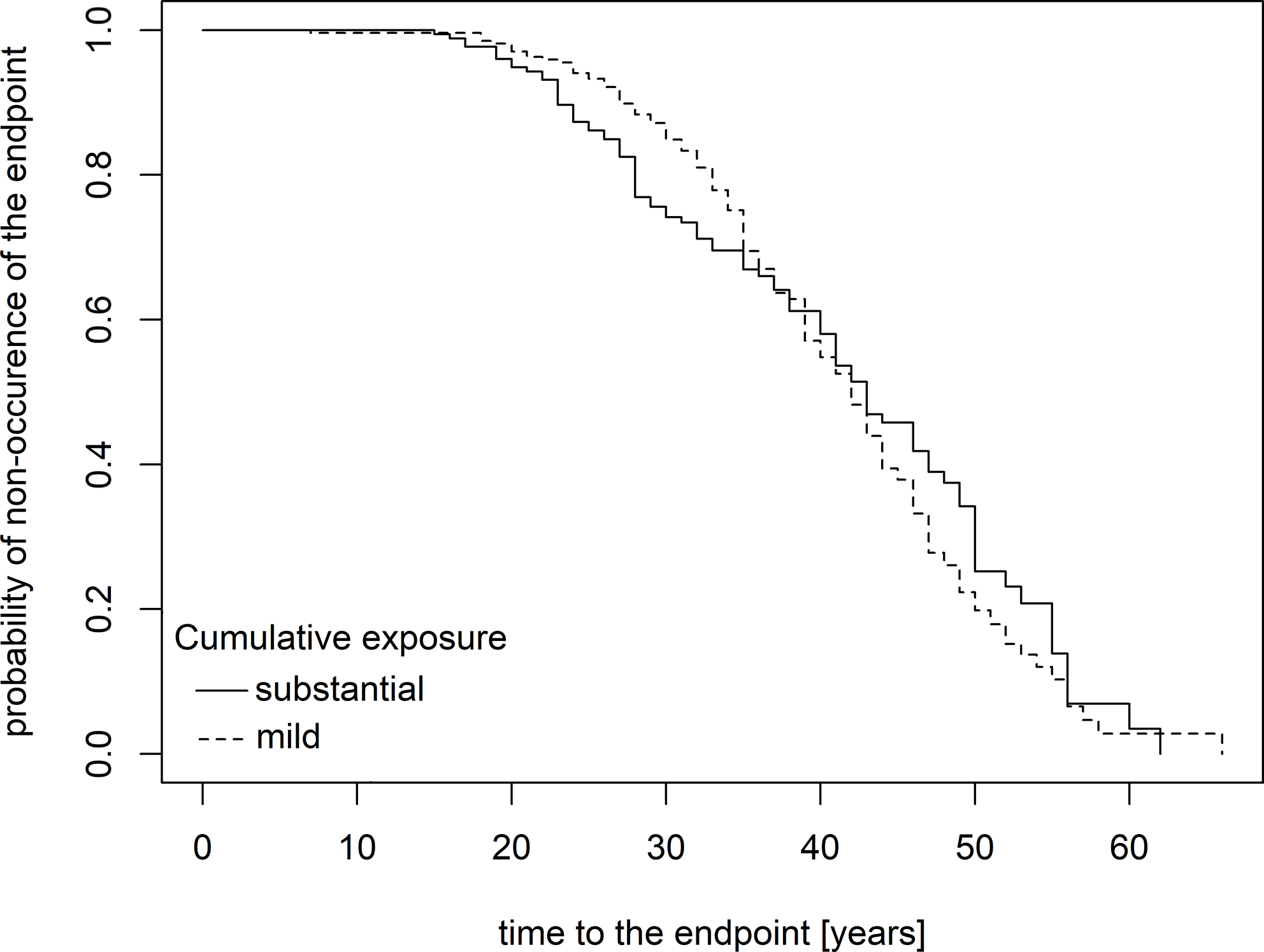
In a sample of individuals with former occupational asbestos exposure, a significant association was observed between cumulative exposure and the subsequent development of pleuropulmonary abnormalities with radiological correlates. Descriptive statistics (Table 1) revealed a gradient in substantial cumulative exposure, highest among individuals with asbestos-related diseases, lower among those with minor radiological findings, and lowest among those without any observed endpoints. Similarly, Cox regression analysis confirmed cumulative exposure as a strong predictor of outcomes (almost double the odds of endpoint in case of substantial exposure). While dust levels did not differ significantly across subgroups, exposure duration exhibited a gradient, increasing from individuals without endpoints to those with asbestos-related diseases. Notably, this trend contrasted with the inverse relationship between exposure duration and outcomes detected in the regression models. This discrepancy may have arisen because descriptive analysis reflected uncensored data (a “best-case scenario”). In contrast, Cox regression accounted for right-censored observations (Bender et al. 2005; Kleinbaum et al. 2012), such as individuals still under follow-up (43.6%) or those whose follow-up ended for reasons other than fatal asbestos-related disease. Despite this, cumulative exposure, as a composite variable incorporating both duration and dust level, consistently emerged as a robust predictor of minor radiological findings and more severe asbestos-associated conditions in both descriptive and regression analyses.
Numerous studies have confirmed a causal link between asbestos exposure and multiple adverse health outcomes, including mesothelioma, lung cancer, hyalinosis, asbestosis, and other cancers (IARC 2012; Loomis et al. 2019). An Italian pooled cohort study on long-term mortality in exposed workers (n = 51,801) demonstrated a statistically significant increase in pleural malignancies depending on cumulative exposure (expressed in fibre-years) in both sexes. Notably, non-malignant chest changes also exhibited this dependence, predominantly appearing in the second and third tertiles of cumulative exposure. Furthermore, a statistically significant excess was observed in cancers of the lip, oral cavity, and pharynx with their incidence increasing across tertiles of cumulative exposure (Magnani et al. 2020). Cumulative asbestos exposure of 25 fibre-years (25 fibres/mL/year) is associated with the onset of asbestosis and approximately doubles the lung cancer risk relative to nonexposed individuals, particularly for mixed fibre types (Klebe et al. 2019). In the current study, substantial cumulative exposure nearly doubled the risk of pleuropulmonary abnormalities. Precise fibre concentration data were unavailable for some participants, as measurements were conducted primarily during occupational disease assessments or workplace inspections by public health authorities, rather than through a systematic monitoring framework. Consequently, dust levels for certain individuals were estimated based on occupational roles and comparable exposure conditions.
Existing evidence suggests that asbestos may also be linked to cardiovascular and autoimmune diseases, further underscoring the need for research extending beyond pleuropulmonary effects to encompass other organ systems (Moitra et al. 2023; Pfau et al. 2014).
The recognition of occupational diseases varies by country. In the Czech Republic, lung, laryngeal, or ovarian cancer can be recognised as an asbestos-related occupational disease only when linked to asbestosis or hyalinosis, with verified workplace asbestos exposure as part of a hygiene survey (Government Reg. No. 290/1995). For example, in Germany, cumulative asbestos exposure of ≥ 25 fibre-years suffices for recognition of lung or laryngeal cancer, even without chest abnormalities (Baur 2018). Our study confirmed cumulative exposure as a key predictor of pleuropulmonary diseases and abnormalities.
PPs are localized areas of fibrous thickening, typically affecting the parietal and diaphragmatic pleura. They usually appear as white or white-tan lesions with a rubber-like consistency but may harden due to diffuse calcification. PP is the most common disorder associated with asbestos exposure and serves as a marker of such exposure (Maxim et al. 2015). In the present study, PP was also the most frequently detected radiological finding. Although benign, PP warrants attention due to its reported association with an increased risk of pleural mesothelioma (hazard ratio [HR] 6.80) (Pairon et al. 2013) and lung cancer (HR 3.13) (Gallet et al. 2022). However, other studies have not established a link between PP and lung cancer (Brims et al. 2020). Despite this plausible association with malignancies, PP is not considered an independent risk factor (Maxim et al. 2015).
In a study by Menant et al. (2024) among 5,392 retired workers occupationally exposed to asbestos in France, the risk of PP grew with increasing cumulative exposure to asbestos adjusted for time since first exposure, age and smoking status. Notably, our results demonstrated a stronger association of cumulative exposure with minor radiological findings than with asbestos-related diseases (OR 1.98 vs. 1.89). Similar to our approach, Menant et al. did not rely on precise dust concentration details for their calculations, as metrology data from the time of exposure were unavailable or atmospheric measurements had not been performed. Instead, they employed a cumulative exposure index in each subject over his working life as the sum of exposures calculated for each exposed job (duration × four weighting factors of exposure intensity). Our study narrowed dust level and exposure duration to binary variables to determine cumulative exposure. This limitation, inherent to the significant time lapse since historical exposures, complicates comparisons between similar studies.
Reaching a correct diagnosis of PP requires a good knowledge of normal locoregional anatomy and a rigorous technical approach to chest imaging examination. The patient’s job history should always be kept in mind (Mazzei et al. 2017). Most frequently, PPs are diagnosed using radiographic methods including chest X-ray or CT. CT scans increase sensitivity and specificity compared to standard X-rays (Maxim et al. 2015), consistent with the higher detection rate of PPs in the subgroup of minor radiological changes by (PET)/CT compared to X-rays in the present study.
Typically, asbestos-induced diseases show a long latency period between the first exposure and the disease diagnosis, often occurring years after the exposure has ceased (Öner et al. 2020). Asbestos-related diseases peaked after a mean latency period of 38 years in Germany (Baur 2018), as in the present sample (Table 1). The latency period for PP is typically reported as 15–40 years (Maxim et al. 2015). In the current study, based on Kaplan-Meier curves, the onset of isolated minor radiological changes appeared to be delayed by several years compared to the onset of asbestos-related diseases.
All asbestos types are carcinogenic, with crocidolite exhibiting a higher malignancy potential than chrysotile (IARC 2012). Asbestos fibres, particularly amphiboles, induce chronic inflammation via inflammasome activation, triggering the release of proinflammatory cytokines. Reactive oxygen species contribute to this process, increasing the risk of inflammation-mediated diseases like mesothelioma, pleural diseases, fibrosis, and lung cancer (Cox 2018). Epidemiological data show higher mesothelioma incidence in crocidolite-exposed cohorts (Beckett et al. 2023). In this study, endpoint analysis—covering malignant, non-malignant, and minor radiological findings—showed no significant association between asbestos type (chrysotile and crocidolite in Plant A vs. chrysotile-only in Plant B) and endpoint occurrence (Tables 1 and 2). This was likely to reflect the composite endpoint approach, which emphasized shared pleuropulmonary abnormalities rather than separating malignancies given the common pathophysiological background.
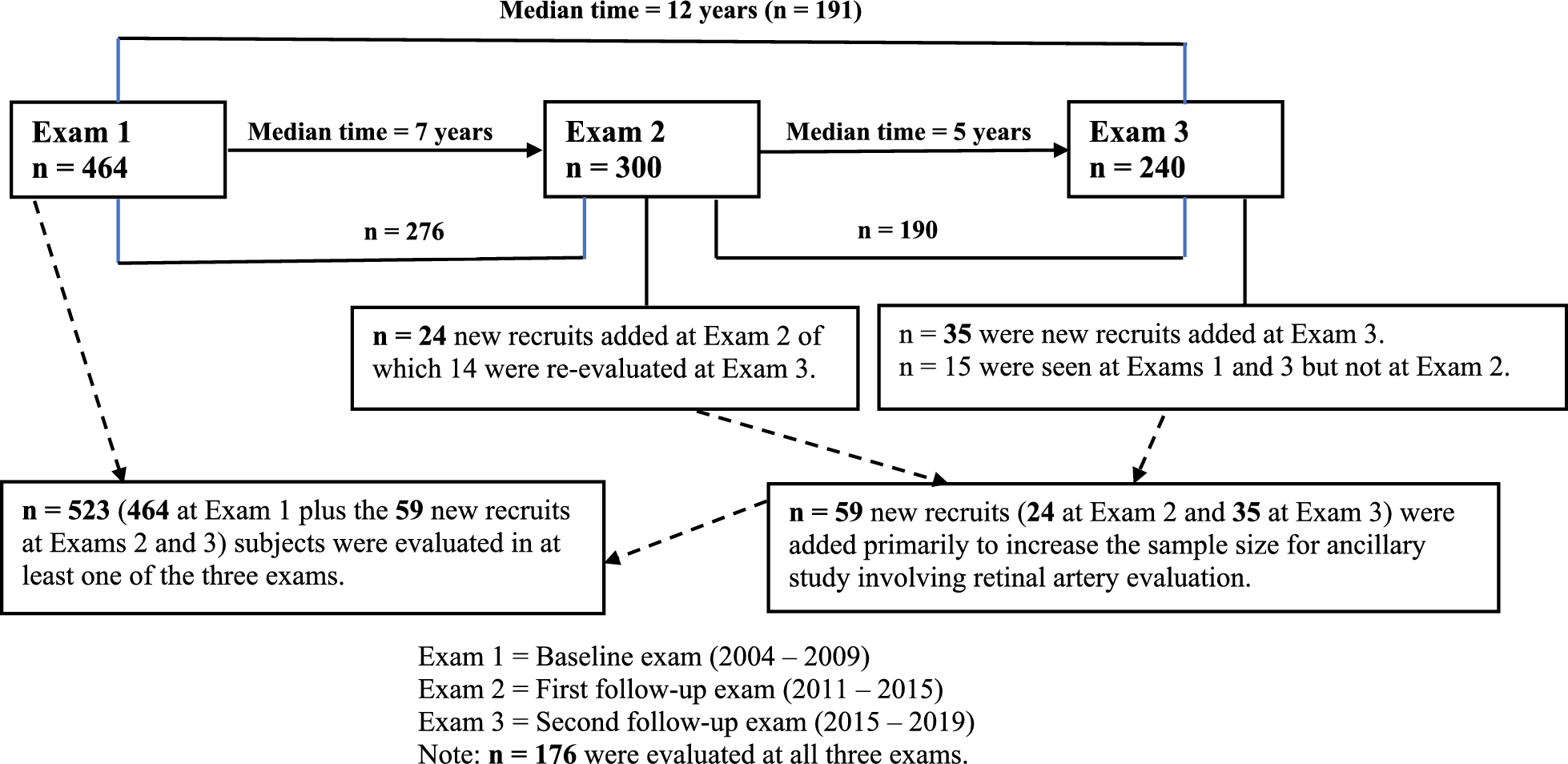
This study has several limitations. Precise asbestos dust concentration data were unavailable for some participants, as workplace dust levels were assessed intermittently during occupational hygiene investigations and did not comprehensively cover all individuals and periods. Cohort heterogeneity is another limitation, as some participants were included through routine post-exposure monitoring while others entered due to suspected occupational diseases. Consequently, selection bias may have occurred, as the study also included referral-based patients, meaning the sample may not be fully representative of the overall workforce in both plants. Additionally, uncertainty arises from potential right-censoring, since reasons for terminating follow-up were not systematically documented. Despite these limitations, the study’s strength lies in its longitudinal design, with participants undergoing regular evaluations usually over several decades, providing robust data on the long-term impacts of occupational asbestos exposure. Additionally, the study population included workers exposed to different types of asbestos. These aspects enhance the study’s contribution to understanding the full spectrum of asbestos-related pleuropulmonary changes.

Comments (0)