
Remember me
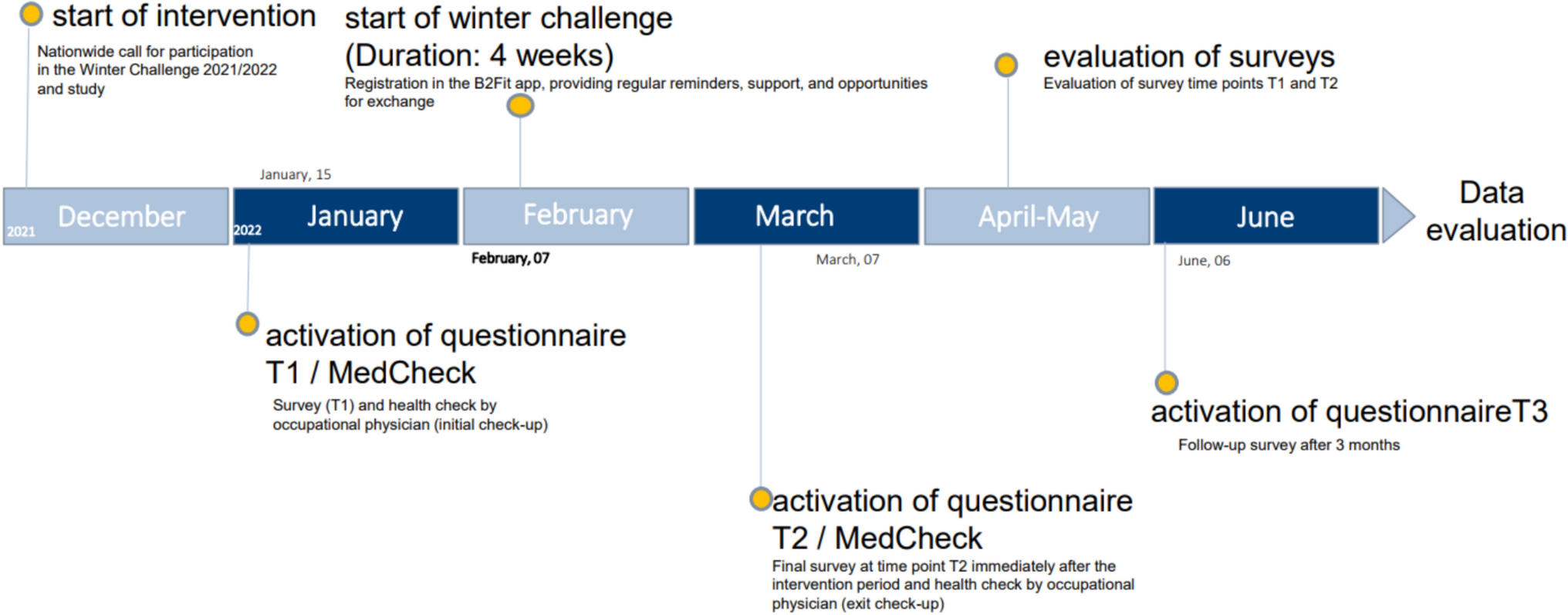
To address the above mentioned research aims, the ‘FC-Fit Winterchallenge 2021/22’ (just called ‘challenge’ in the further text) was process-oriented, externally monitored and scientifically evaluated. Therefore, a quantitative online questionnaire was administered to the participants prior to (T1), directly after (T2), and three months after (T3, follow-up) the four week challenge. In addition, employees had the opportunity to undergo a health check-up with the responsible company medical officer at T1 and T2. During this check-up, cardiovascular data, body measurements, and blood values such as glucose and blood lipids were assessed. However, the results of this check-up are not included in the present paper, which focuses on the results of the quantitative survey.
The start of the challenge was launched in December 2021 with a nationwide announcement to all employees of the DHL Group. The challenge was promoted using the companies’ internal newsletter, the website, and with posters that were placed at the company’s headquarters in Bonn. To participate in the challenge, employees had to register in the app. During this process, a personal ID was generated and sent to the employees of the DHL Group by e-mail. As part of the challenge, the app was used to increase health awareness. For this purpose, a points system was used to reward healthy eating, physical activity, and mindfulness.
The survey was performed using the open source software ‘LimeSurvey’. It could be accessed at all time points by using an ID, which was generated during initial registration in the app. Approval to perform the study was obtained by the ethical committee of the Medical Association of Rhineland-Palatinate (application number: 2021-16233). The study was performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans and the Ethical Principles and Guidelines for the Protection of Human Subjects of Research by the American Psychological Association (APA). A monetary donation to a charitable organization was used as an incentive to increase the likelihood of participation by triggering emotional responses, as recommended, for example, by Gendall and Healey (2010) and others (Reichel et al. 2021). Specifically, it was offered that if 1000 participants completed the survey, €1000 would be donated to the Children’s Cancer Aid Foundation (German: Stiftung Deutsche Kinderkrebshilfe).
In the online survey, at T1, sociodemographic and work-related characteristics as well as various health-related constructs (described in detail below) were assessed. At T2 and T3, only the health-related constructs were further assessed to examine the effect of the challenge on health over time (Fig. 1).
Fig. 1 Measures
MeasuresAt T1, the survey included 45 questions. Whenever possible, established and validated measurement instruments were used. An overview of all questions used in the present survey is appended to this paper (Appendix 1). With regard to the first research aim, namely to investigate the effect of the challenge on somatic symptoms and to evaluate whether potential effects differ with regard to sociodemographic and work-related variables, the dependent variable somatic symptoms was assessed using the PHQ-15 questionnaire. It is a module for recording somatic symptoms as part of the Patient Health Questionnaire (PHQ) and suitable for measuring the severity of somatic symptoms and the severity of somatoform disorders. This is possible because no organic explanation of the symptoms is assumed for the evaluation (Kroenke et al. 2002; Stauder et al. 2021). This makes it useful in clinical practice as well as in the scientific consideration of mental and physical health. It includes the most common somatic symptoms (excluding upper respiratory symptoms) of outpatients, representing over 90% of reported physical complaints, and implements two additional questions on sleep disturbance and fatigue/energy loss. The self-report of the participants is possible on a scale of 0 (not bothered at all) to 2 (bothered a lot). In the scoring of the PHQ-15, values from 0 (no somatic symptoms) to 30 (severe somatic symptoms) can be obtained. In this context, values from 0 to 4 indicate minimal somatic symptoms. Values between 5 and 9 are interpreted as mild somatic symptoms, values between 10 and 14 are an indication of moderate somatic symptoms and scores of 15 and above are indicative for severe somatic symptoms (Kroenke et al. 2002).
In addition to sociodemographic and work-related variables, which are listed in Table 1 with their respective distributions and mean values for all three time points, the variable groups ‘health-related behavior’ and ‘mental health’ were also assessed. Referring to health-related behavior, the short form of the International Physical Activity Questionnaire (IPAQ-short) was used to measure physical activity (Sember et al. 2020) and the Alcohol Use Disorders Identification Test (AUDIT-C) to measure alcohol consumption. The AUDIT-C is an abridged version for the assessment of alcohol use disorders. It has been developed by the World Health Organization (WHO) and is one of the most common screening instruments for harmful and hazardous alcohol use worldwide (Babor and Robaina 2016). Additionally, the questions regarding cigarette and painkiller consumption were self-developed, with the response options adapted to the common vocabulary of scale items. For mental health variables, validated measurement instruments were used, including for burnout (COPSOQ-B13), anxiety and depression (PHQ-4), as well as stress (PSS-10). The COPSOQ-B13 is the burnout question module from the COPSOQ (Copenhagen Psychosocial Questionnaire). It is a scientifically validated questionnaire for the assessment of psychological resilience at work. In different studies, the quality criteria such as generalizability, construct validity or critical validity could be confirmed (Nübling et al. 2005). The PHQ-4 is an ultra-brief screening scale for anxiety and depression in the Patient Health Questionnaire (PHQ). It consists of the two questions from the PHQ-2, used to screen for depression, and the two questions from the GAD-2 (Generalized Anxiety Disorder), which is used to screen for general anxiety. The PHQ-4 has scientifically accepted construct validity and can be used as a general marker of psychological distress (Kroenke et al. 2009). The Perceived Stress Scale (PSS-10) is a widely used measurement scale for perceived stress. It is associated with depression, anxiety, lower life satisfaction, and lack of motivation. Here, the ability to cope with stress and the perceived excessive demands of everyday life will be questioned (Cohen et al. 1983; Klein et al. 2016).
Table 1 Sociodemographic and work-related characteristics of study samplesStatistical analysisThe description of the statistical analyses will be divided into two parts, based on the two study aims.
With regard to the first study aim, namely to investigate the effect of the challenge on somatic symptoms and to evaluate whether potential effects differ with regard to sociodemographic and work-related variables, descriptive results are presented as means with standard deviations (SD). To compare values between T1 and T2 as well as T2 and T3, paired t-tests were used if the conditions that apply for this analysis were fulfilled. Results are presented with T-values, effect sizes (d) and p-values (p). To investigate potential differences in means between subgroups, paired t-tests were performed if there were two values in the relevant subgroup, the variables were normally distributed, or had a minimum of 30 samples in each value. When these conditions could not be met, Mann–Whitney-U-test (U) with Z-statistic (Z) was used for the analysis of these subgroup comparisons. For variables with more than two values, Kruskal–Wallis-test (X2) was used. When considering the longitudinal differences for each subgroup, Wilcoxon-Signed-Rank-test (z) with the effect size (r) was applied. All analyses were checked additionally with parametric tests in order to secure the results.
To address the second aim of the study, namely to investigate potential predictors of somatic symptoms among employees of the Deutsche Post DHL Group, a linear multiple regression analysis was performed with the data of T1 using the PHQ-15 score as dependent variable. The T1 sample was chosen for the multiple linear regression because at T1, the sample size was sufficient compared to T2 and T3. With a general population of around 225,000 employees of the Deutsche Post DHL Group in Germany, a priori power analysis revealed a sample size of at least 384 cases for the regression analysis. A confidence level of 95% and a margin of error of 5% were assumed.
The sociodemographic independent variables were included in the regression analysis as follows: Age was treated as a metric variable but not centered at the mean, as the study registration criteria already specified that participants had to be adults, and the maximum age was capped at 65 years. With regard to the binary variable gender, ‘male’ is the reference category. The variable educational degree was recoded to a dummy variable representing a binary variable having the general qualification for University entrance or not. Here, the category ‘no’ is the reference category. With regard to the work-related independent variables, the variable working time model was divided into full-time and part-time employment, with part-time employment as the reference category. The variable work area was recoded as a dummy variable. It is now indicating if the participants work in the administration sector or not with the reference category ‘no’. The recoding into dummy variables was necessary because a comparison between the subgroups was not possible due to strongly differing case numbers. Finally, with regard to the variable type of job, the category ‘predominantly mental’ was used as a reference, contrasted with the categories ‘predominantly physical’ and ‘equally mental and physical’. Referring to variables on health-related behavior, the variables alcohol, cigarette and painkiller consumption were recoded into dummy variables, with the category ‘no’ being used as the reference for each variable. The variable physical activity was divided into the categories ‘insufficiently active’, ‘moderately physically active’, and ‘highly physically active’, with insufficiently activity being the reference category in each case. The independent variables associated with mental health were integrated for the regression analysis as follows: The Perceived Stress Score (PSS-10) and the Burnout Score (COPSOQ B13) were used as metric scaled variables. Depression (PHQ-2) and Generalized Anxiety Disorder (GAD-2) were recoded into dummy variables according to their specific cut-off values. The negative screenings are considered the reference category in each case. The test for multicollinearity, conducted through a correlation matrix (Urban and Mayerl 2018), variance inflation analysis, and the calculation of VIF values, indicates that the independent variables used are not exhibiting linear dependency on each other. In the residual analysis for homoscedasticity both the significant White test and the significant Breusch-Pagan/Cook-Weinsberg test suggest a violation of the homoscedasticity assumption, indicating heteroscedasticity. However, in such instances, the standard errors of the coefficients may become biased, potentially leading to erroneous assumption of significant effects. To address this, bootstrapping can be employed to mitigate heteroscedasticity. For this reason, bootstrapping with 1000 samples was performed in the regression analysis. Testing for normal distribution of the residuals, the histogram and PP-plot show an approximate normal distribution. The skewness and kurtosis of the studentized residuals were smaller than the cut-off ranges reported in the literature (MRC Cognition and Brain Sciences Unit 2018), therefore, normal distribution could be assumed. The statistical analyses were performed using IBM SPSS version 27.
In addition, mean comparisons were performed between T1 and T2 as well as T2 and T3 for the independent health-related variables that had significant regression results. These were performed using a paired t-test (t), analogous to the treatment of the first aim of the study, if the precondition test was met (t, d, p). If the precondition test was not fulfilled, the results could be tested with the nonparametric Wilcoxon-Signed-Rank-test (z, r, p).
Comments (0)