
Remember me
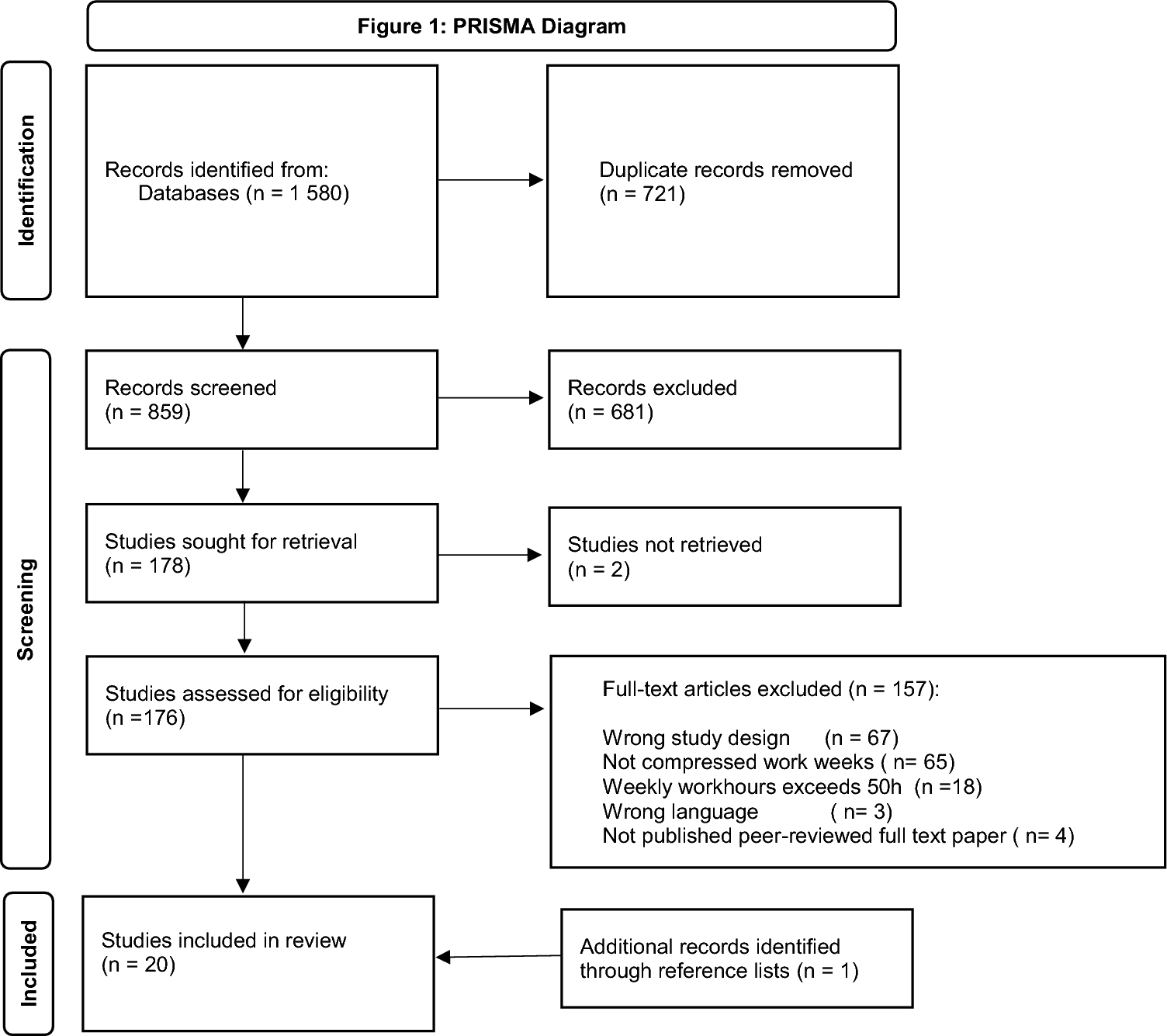
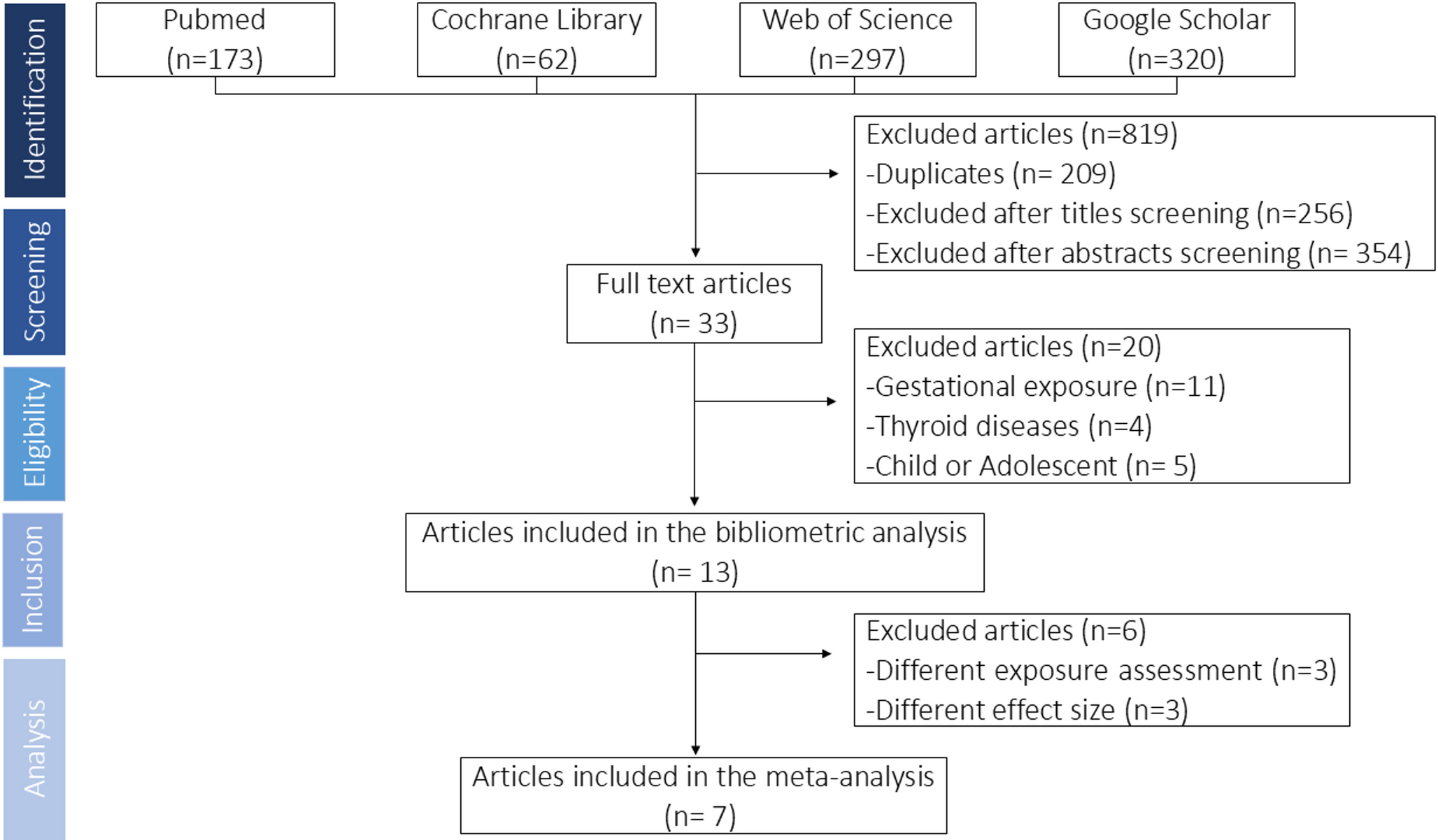
The database search resulted in 1580 references, as presented in Fig. 1. After excluding duplicates, 859 abstracts were screened by two independent researchers, of which 176 studies were also screened in full text. One additional study was included from reference lists in the included studies. Finally, 20 studies (see Table 2) met the inclusion criteria.
Table 2 Summary of studies included in the systematic analysisAll studies were published in English between 2005 and 2022. Sample sizes ranged from 39 to 21 440. Most of the 20 studies examined health care workers (n = 8) or industrial workers (n = 5), with the rest examining workers within the police (n = 3), technology (n = 2) and airport (n = 1). One study examined compressed workweeks in the general working population. The studies were from Europe (n = 8), North America (n = 6), Asia (n = 5) and The Middle East (n = 1). The study design was longitudinal designs with follow-up intervals varying from 4 weeks to 10 years.
Of 20 studies, 15 studies investigated outcomes related to employee health and wellbeing (Table 3), and 8 studies related to work safety and performance (Table 4). See Table 5 for the results of the quality assessment of the included studies. Below we synthesise the evidence based on the type of outcome, shift length and work hours in the control group, and summarize the quality of evidence. The evidence synthesis based on outcome is illustrated in Fig. 2 (health and wellbeing) and Fig. 3 (safety and performance).
Table 3 Health outcomes related to compressed work schedulesTable 4 Safety and performance outcomes related to compressed work schedulesTable 5 Quality assessment of studies based on EPHPP criteria: Total score and quality according to component ratingsFig. 2 Fig. 3
Fig. 3
Evidence map job outcomes
Health and wellbeing outcomesAmong the 15 studies investigating health and wellbeing outcomes, 11 studies compared a compressed schedule to an 8 h schedule, 3 studies investigated extended shifts while controlling for weekly work hours, and one study compared two different compressed schedules (3 days of 13.5 vs 4 days of 10 days). The most frequently investigated health outcomes were sickness absence and sleep, with a total of 6 studies investigating each outcome. The results are illustrated in Fig. 2 (sorted by quality of evidence and including only outcomes investigated in at least two studies).
In sum, the results were mixed. Of 15 studies, 11 reported at least one significantly negative health or wellbeing outcome of a compressed schedule or extended shifts, 10 studies reported at least one non-significant outcome, and 6 studies reported at least one significantly positive outcome. Of the outcomes examined in multiple studies we found moderate support for compressed schedules being beneficial for satisfaction with work schedule. We found moderate support for compressed schedule (and particularly extended shifts (≥ 12 h) controlled for weekly work hours) being detrimental in terms of sickness absence. For all other health and wellbeing outcomes the results were either mixed or insufficient for conclusions.
Reviewing the specific outcomes in more detail; of the seven studies investigating sickness absence, two found no significant difference, four found higher absence among the compressed workers and one compared two different compressed schedules. The two studies which found no significant differences both compared a compressed schedule with 12 h shift to a non-compressed schedule (Amendola et al. 2011; Battle and Temblett 2018b), one of the studies also included a 10 h shift schedule (Amendola et al. 2011). Of the four studies that found higher absence rates, one compared a compressed 12 h shift schedule to an 8 h shift schedule (Rodriguez Santana et al. 2020), two investigated extended shifts (≥ 12 h) controlled for weekly work hours (Dall'Ora et al. 2019; Ropponen, Koskinen, Puttonen, & Harma, 2020), and one investigated self-reported compressed work schedules without specifying length of shift (Dionne and Dostie 2007). The last study compared two different compressed schedules (13:20 h × 3 days vs 10 h × 4 days) and found no significant differences (Bell et al. 2015). Because Bell et al. (2015) compares two compressed schedules this study is not included in the evidence synthesizing using the EPHPP-global rating. Overall, there is moderate support that compressed work schedules are longitudinally linked with higher sickness absence, according to the EPHPP-global rating.
Of the six studies investigating sleep, all have included different sleep related outcomes, most commonly sleep quality, sleep amount, and sleepiness.
One study found partial support for better sleep quality (Shochat et al. 2019), while two studies found no significant difference in sleep quality (Amendola et al. 2011; Casjens et al. 2022a), all examining compressed 12 h shift schedule versus non-compressed shifts. Moreover, one study also found no significant difference in sleep quality when examining a compressed 10 h shift schedule versus non-compressed shifts (Amendola et al. 2011). A fourth study compared two different compressed schedules and found poorer sleep quality when employees work 13.5 h shifts rather than 10 h shifts (Bell et al. 2015). There is insufficient evidence to support a longitudinal relationship between compressed work and sleep quality, according to the EPHPP-global rating.
Investigating sleep amount, two studies found that employees reported more sleep in total when working a compressed 12 h (Shochat et al. 2019) and 10 h schedule (Amendola et al. 2011) versus a non-compressed schedule. The difference was not significant when sleep was measured objectively by actigraphy in one of these studies (Shochat et al. 2019). Two studies found no significant difference in total or habitual sleep, but they found significant differences when dividing sleep according to shift type and work-free days (Casjens et al. 2022b; Puttonen et al. 2022). More specifically, one study found that employees working a compressed schedule with 12 h shift, compared to a non-compressed schedule, slept more on work-free days, but less on workdays, yielding insignificant difference on total sleep (Casjens et al. 2022a). The other study found that employees on compressed schedules of 12 h shift slept more before and between morning shifts compared to employees on a non-compressed schedule, but not on any other day (Puttonen et al. 2022). Finally, one study found more sleep when employees worked a compressed schedule of 10 h shifts compared to a compressed schedule of 13.5 h shifts (Bell et al. 2015). There is mixed evidence for a relationship between compressed work and sleep amount.
Four studies investigated sleepiness, alertness and daytime disfunction. Two studies found partial support for less sleepiness (Puttonen et al. 2022; Shochat et al. 2019) while another found significantly more sleepiness and less alertness (Amendola et al. 2011) when working a compressed 12 h schedule, as compared to a non-compressed schedule. Comparing two compressed schedules, a fourth study found more daytime dysfunction due to sleepiness (e.g. having trouble staying awake) when employees work 13.5 h shifts rather than 10 h shifts (Bell et al. 2015). There is mixed evidence for a relationship between compressed work and sleepiness.
Of additional sleep related outcomes two studies found no significant difference in sleep disorder between a compressed 12 h schedule, 10 h schedule and non-compressed schedule (Amendola et al. 2011) or insomnia for a compressed 12 h schedule compared to a non-compressed schedule (Puttonen et al. 2022). One study found that employees working compressed 12 h shifts had significantly more social jetlag (i.e. a larger difference in sleep patterns between work and free days) (Casjens et al. 2022b).
Four studies investigated stress and work pressure. Of these, two studies found no significant difference in stress measured with cortisol levels between 12 and 8 h shift workers, (Casjens et al. 2022a) or between 13 and 10 h shift workers (Bell et al. 2015). One study found no significant difference in work-related stress measured with self-reports between 12 h, 10 h and 8 h shift workers (Amendola et al. 2011). One study found significant higher self-reported work pressure for employees working a compressed schedule of 12 h (Bacon et al. 2005). There is insufficient evidence to support a relationship between compressed work and stress and work pressure. Rather, with three strong or moderate studies reporting no difference in stress or work pressure, the evidence could be interpreted as moderate support for there not being a relationship. However, it is important to note that none of the studies used non-inferiority tests or equivalent approaches to directly assess the certainty of the null hypothesis (i.e. that there is no difference).
Three studies investigated quality of work life, job satisfaction and satisfaction with shift system. All studies reported positive results for a compressed schedule. The results included higher satisfaction with this shift system (Puttonen et al. 2022) and a higher satisfaction with working hours, shift rotation pattern and overall job satisfaction (Bacon et al. 2005) among employees working a compressed 12 h shift schedule compared to a non-compressed schedule. In addition, employees working a compressed 10 h shift schedule reported better quality of work life (measured as job satisfaction, schedule satisfaction, organizational commitment, and job involvement) compared to a non-compressed schedule (Amendola et al. 2011). In accordance with the EPHPP-global rating, there is moderate evidence that compressed work schedules are longitudinally linked with higher satisfaction with shift system.
Three studies investigated quality of life or work-life balance. One study found significantly improved work-life balance among employees working a compressed 12 h schedule (Puttonen et al. 2022). Another study reported no significant differences in self-reported quality in personal life (measured as work-family conflict) when working a compressed 12 or 10 h schedule compared to a non-compressed schedule (Amendola et al. 2011). A final study reported significantly lower quality of life among employees working a compressed schedule with 13.25-h shifts compared to employees working 10 h shifts, and no significant difference in partners’ quality of life (Bell et al. 2015). The evidence for work-life balance is insufficient.
Two studies investigated burnout—both supporting less burnout among employees working compressed 12 h work schedules (Battle and Temblett 2018b; Shochat et al. 2019). With one study rated as weak and one moderate—the evidence for burnout is insufficient.
Two studies investigated cardiovascular health, with one study finding no significant difference in cardiovascular health between compressed 12 h, 10 h and a non-compressed schedule (Amendola et al. 2011) and the other finding increased risk of metabolic syndrome for employees working compressed 12 h work schedules (Oh and Yim 2018). The evidence for cardiovascular health is therefore mixed.
Finally, certain outcomes were only investigated in one study supporting negative consequences for health outcomes including menstrual cycle irregularities (Su et al. 2008) and musculoskeletal disorder (Trinkoff et al. 2006), while others reported no significant differences for gastrointestinal problems (Amendola et al. 2011), personal injuries (Battle and Temblett 2018b), subjective health, work ability, and need for recovery (Puttonen et al. 2022).
Safety and performance outcomesIn all, eight studies investigated safety or performance outcomes of compressed work weeks. The outcome measures were diverse. Several studies focus on sector-specific outcomes, particularly outcomes in the healthcare sector and police force. The results are illustrated in Fig. 2 (sorted by quality of evidence).
In sum, the studies revealed mixed results for the safety and performance consequences of compressed workweeks when outcomes are grouped together. The level of evidence for each individual outcome is insufficient—with few studies investigating the same outcome. Two studies reported significantly positive outcomes (Tanaka et al. 2010; Wijaya et al. 2020), and one studies reported significantly negative outcomes (Barnum 2011). And one study reported mixed results when comparing compressed shifts of different lengths (Bell et al. 2015). Most studies found some insignificant outcome measures.
Reviewing the specific outcomes in more detail; four studies investigated safety and performance outcomes of compressed workweeks within the healthcare setting. Two studies found beneficial outcomes for patient safety; including improved patient safety culture when comparing a compressed schedule of 12 h shifts to 8 h shifts (Wijaya et al. 2020) and reduced risk of error in patient care when comparing a compressed schedule of 9 h day and 16 h night to a schedule of 8 h day and 10 h night (Tanaka et al. 2010). Two other studies found no significant differences in clinical incidences (i.e. events that could have, or did result in, unnecessary harm) (Battle and Temblett 2018b) and the rate of x-ray images taken by radiographers that had to be rejected (Ooi et al. 2021) when comparing a compressed schedule with 12 h shifts to a non-compressed shift schedule. Both studies supporting positive effects of a compressed workweek on patient safety relied solely on self-report. There is mixed evidence for whether a compressed work schedules is longitudinally linked with healthcare outcomes. Though mixed, findings are positive or non-significant, and there are no studies supporting negative health care outcomes of compressed workweeks.
Three studies investigated safety or performance outcomes of compressed workweeks in the police force. All three studies included some measure of activities completed. One study found no significant difference in activity levels (e.g. arrests made) between 12, 10 and 8 h shifts (Amendola et al. 2011). The second study found significant longer time for answering calls during 12 h shifts compared to 8 h shifts, but no other significant difference in time spent handling calls (Barnum 2011). The third study found that police officers working 13 h shifts conducted significantly more adult bookings (i.e., the processing of individuals taken into custody) and field interrogations compared to those working 10 h shifts (Bell et al. 2015). There is mixed evidence for whether a compressed work schedule is longitudinally linked with activities completed withing the police force.
Two of the studies investigating safety or performance in the police force also included performance on test and simulations, one comparing a comparing two compressed schedule of 12 h and 10 h shifts to an 8 h hour shift schedule (Amendola et al. 2011) and one comparing between 13 and 10 h schedules (Bell et al. 2015). The studies did not find a significant difference in police officers´ results on shooting tests between any of the schedules (Amendola et al. 2011; Bell et al. 2015) or on a driving simulator (Amendola et al. 2011). One study found no significant difference on vigilance or fatigue test (Amendola et al. 2011), while another study showed mixed results of the vigilance test as officers working 13 h shifts demonstrated significantly more lapses in concentration compared to officers on 10 h shifts, but also fewer anticipatory errors at one point after the intervention (Bell et al. 2015). The latter study examining vigilance also found no significant difference between 13 and 10 h shift schedules in cognitive processing at the beginning of a shift, but significantly poorer cognitive processing at the end of shift among officers working the longest shifts (Bell et al. 2015). Additionally, they found that officers working the 13 h shift schedule had a significant increase in number of citizen complaints, and involvement in incidents (Bell et al. 2015). There is not sufficient evidence to assess whether a compressed work schedule is longitudinally linked with performance on test and simulation.
Finally, as the only study investigating safety and performance outcomes outside the health and police sectors; investigating senior executives in a technology company, Mills and Grotto (2017) found no significant relationship between self-report of working compressed workweeks and supervisor-rated performance.
Summarizing all findings by shift length and work hours in control groupsHere we summarize all findings about the consequences of compressed workweeks by the shift leng
Comments (0)