Our study, representing one of the largest cohorts of AML long-term survivors studied so far, reveals that QoL of AML LTS five or more years after the initial diagnosis, on average, reaches levels comparable to adults without a history of cancer. Similar results were found in a longitudinal study that examined QoL in intensively treated AML patients for three years after their initial diagnosis, with almost 80 percent reporting “normal” QoL [27]. Since other studies with shorter follow-up reported impaired QoL [7], this may indicate that QoL of survivors recovers over several years after diagnosis and treatment of AML. However, no association between time since diagnosis beyond 5 years and QoL was identified in our study, similar to a prior large study including various blood cancers [28].
Even though many AML survivors reported good QoL, one in four long-term survivors still experience meaningful impairment even ≥5 years after initial diagnosis. Like overall QoL, most secondary outcomes evaluated in our study also showed a skewed distribution (Supplementary Fig. S3), indicating that a substantial minority of survivors have lasting impairment and might benefit from additional support. We were able to identify factors associated with long-term impairment of QoL and health satisfaction, including a change in occupational status, a higher degree of disability, higher number of comorbidities, and higher fatigue and anxiety levels. On the other hand, we also identified protective factors including older age, better social support and a bigger household size, which in part align with previous research [8]. Likewise, a prior, single-center study of 5-year survivors of various hematological cancers identified medical comorbidity, psychological distress, lower social support, and high levels of fatigue and functional impairment as factors associated with a stronger negative impact of cancer on subsequent quality of life [29]. Of note, in this study, acute leukemia survivors scored significantly higher on the scales measuring positive impact of cancer (e.g., on the positive self-evaluation and health awareness scales of the Impact of Cancer Questionnaire) compared to survivors of other entities, in agreement with the favorable overall outcomes seen in our cohort.
While some socio-demographic factors for impaired QoL such as younger age and lower levels of social support cannot be directly influenced by the medical care team, they identify individuals at a greater risk for impairment in QoL who may benefit from more intensive psychosocial support. Even though a significant proportion of cancer survivors reportedly show resilience or post-traumatic growth, younger age has been reported as a risk factor for adverse survivorship outcomes across cancer entities [30]. Complex interactions of various factors, such as being diagnosed during particularly sensitive life stages (e.g. while establishing financial security, developing an own identity, or raising a family), as well as negative peer comparisons due to impacts of the disease and its treatment may contribute to this effect. Additionally, some risk factors such as changes in occupational situation, which had a strong impact on QoL in our study, may particularly affect younger survivors. Another large German study showed that more than a third of former blood cancer patients had not returned to work ≥3 years (median, 9 years) after their initial diagnosis [28]. Consequently, QoL might be positively impacted through targeted occupational programs addressing these aspects.
Our study also evaluated life satisfaction of survivors. In contrast to QoL, LS captures a person’s individual perception of how far their life quality matches a self-imposed standard [31]. LS has been rarely addressed in prior research on AML survivors [11]. We were able to differentiate between gLS and hrLS, and identified specific factors associated with favorable or unfavorable outcomes for each domain. Overall, life satisfaction was less commonly impaired than QoL, indicating that some survivors were satisfied with their current life situation even in the presence of a significant symptom load captured by the QoL instruments. This finding, as well as the mostly favorable QoL outcomes in our cohort, might be explained by “response shift”, which describes the phenomenon that the meaning of some constructs and items in patient-centered outcome measures is time dependent, and patients may interpret them differently as they go through new life experiences [32]. Potential mechanisms of response shifts include recalibrating (i.e., survivors may have adopted a novel reference frame due to the experiences made during their disease), reprioritizing (i.e., a change in the importance of different components in the target), reconceptualizing (i.e. redefining the construct altogether) or a combination of these. This points to life satisfaction being an important outcome in survivorship research.
Figure 4 shows a network diagram integrating our results on factors that positively or negatively affect QoL and LS of AML survivors. It highlights a key strength of our study: our multi-dimensional approach that captures different aspects of survivorship outcomes, as well as a broad range of potentially impacting factors. Overall, physical fatigue emerged as the only factor associated with worsening of all three primary outcomes, while better social support was a protective factor for all three. Other factors affecting hrLS (e.g., anxiety, comorbidity burden, and physical fatigue) were also relevant for QoL, suggesting interventions addressing them could benefit both domains.
Somatic comorbidities were associated with impaired QoL and hrLS. AML survivors in our study had a mean of 2.3 comorbid conditions captured by the FCI score. In a recent study, 2-year survivors of allogeneic transplantation had a 3.8-times higher risk of severe or life-threatening conditions compared to their siblings [33], also emphasizing the importance of addressing late and long-term morbidity as an underlying cause for long-term impairment of QoL. Screening for medical comorbidities and treatment of the associated symptoms may not only help to improve QoL in AML LTS but also improve late mortality that has been observed in young AML survivors [34].
Notably, treatment modality (i.e., whether a patient had received an allogeneic transplantation or only cytotoxic chemotherapy) did not consistently associate with QoL or LS and in particular, allogeneic transplantation or a prior disease relapse did not correlate with poorer outcomes among our participants (Supplementary Table S8). Indeed, survivors who had undergone alloHSCT reported better hrLS than participants treated with chemotherapy alone. Again, response shift due to re-calibration of patients’ expectations after the experience of undergoing alloHSCT may be one factor contributing to these favorable self-reported outcomes. Alternatively, survivors suffering from severe transplant-induced LLTE, such as chronic GvHD, might have been less willing to participate in our study or may have been more likely to die before the 5-year landmark. However, such a selection bias would be unlikely to completely eliminate or even reverse any between-group differences.
While QoL and hrLS shared a subset of overlapping associated factors that may be long-term consequences of leukemia and its treatment, gLS was linked to a different subset of factors such as household income or having children, which are only partly linked to the disease. Thus, general life satisfaction seems to be only weakly affected by AML-related factors in long-term survivors.
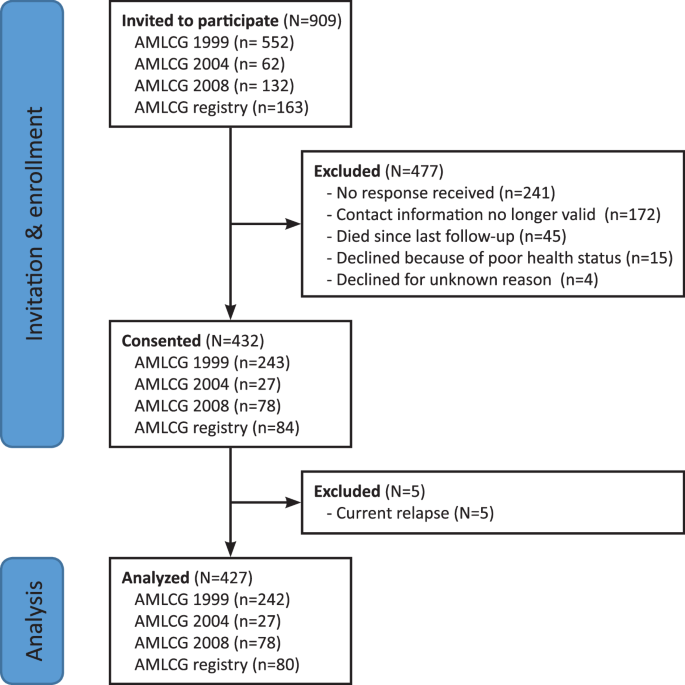
Strengths of our study include its large cohort size, multicentric recruitment, and our multi-dimensional approach. We focused on a single entity and only included survivors in remission, since prior studies in mixed population have revealed differences in survivorship outcomes between different entities [28]. On the other hand, we included survivors across a broad age range and did not restrict our analysis to a specific treatment modality, such as allogeneic transplantation. Overall, we believe our data are representative of AML survivors in Germany. Our study also has limitations. Although we used repeated contact attempts to achieve a high response rate, we cannot fully exclude non-responder bias. However, the response rate of 63% can be considered very high for a study enrolling former patients from multiple centers 5 to 18 years after diagnosis and exceeds the previously recommended threshold of 60% for oncology patient surveys [35]. As pointed out by Nishimura et al. [36], response rates are not well-suited to assess non-responder bias. Comparing data from responders and non-responders using available baseline data (collected at diagnosis) did not reveal any severe or unexpected differences, but this only provides an indirect assessment of potential non-responder bias. Other statistical approaches to diagnose or adjust for non-response bias also have weaknesses [36]. The possibility that participants with strongly impaired QoL – or, vice versa, particularly good QoL- might have preferentially declined participation in our study therefore remains. On the other hand, despite our cohort’s particularly long follow-up, the response rate in our study compares favorably to previously reported cohorts of AML survivors (44–69%), supporting the generalizability of our findings [7, 8, 10, 11, 16, 29, 31, 33]. Due to our cross-sectional approach, we did not collect information on intra-individual trajectories of QoL and LS over time. We used the FACT-G overall score as a comprehensive and robust instrument capturing multiple domains of QoL within a single summary score as part of our primary endpoint. Available FACT-G normative data were derived from an Austrian population sample, which, although originating from a neighboring, culturally similar and German-speaking country, might have introduced bias. However, analysis of the EORTC QLQ-C30 Global Health Status score using contemporary German normative data yielded results consistent with the FACT-G summary score. Lastly, our multivariable analysis for impaired QoL and LS revealed a strong intercorrelation between psychosocial variables and the primary outcomes, which may hamper identification of other relevant associations. Further research is warranted to identify causal relationships that impact survivorship outcomes, and that might be addressed in risk-adapted survivorship care programs.
In conclusion, our study presents long-term outcomes from one of the largest cohorts of acute leukemia survivors. Patients and physicians battling this disease should be reassured by our finding that QoL and LS of many AML LTS are comparable to reference populations without leukemia. Importantly, however, a subset of survivors continues to experience impaired global QoL even ≥5 years after their initial diagnosis. Furthermore, AML LTS show persistent impairment in several specific domains of QoL, such as social functioning. Collectively, these data highlight the need to include guidance for structured follow-up care into clinical guidelines [37]. Our data identify relevant problem fields of AML survivors that should be subject of further studies, and that might be modified by targeted interventions. As many cancer survivors, and especially those with a perceived disease-related burden, are dissatisfied with their medical care [38], our data may provide a foundation to develop improved, needs-based and risk-adapted survivorship care models for AML LTS beyond the five-year mark after diagnosis.


Comments (0)