
Remember me
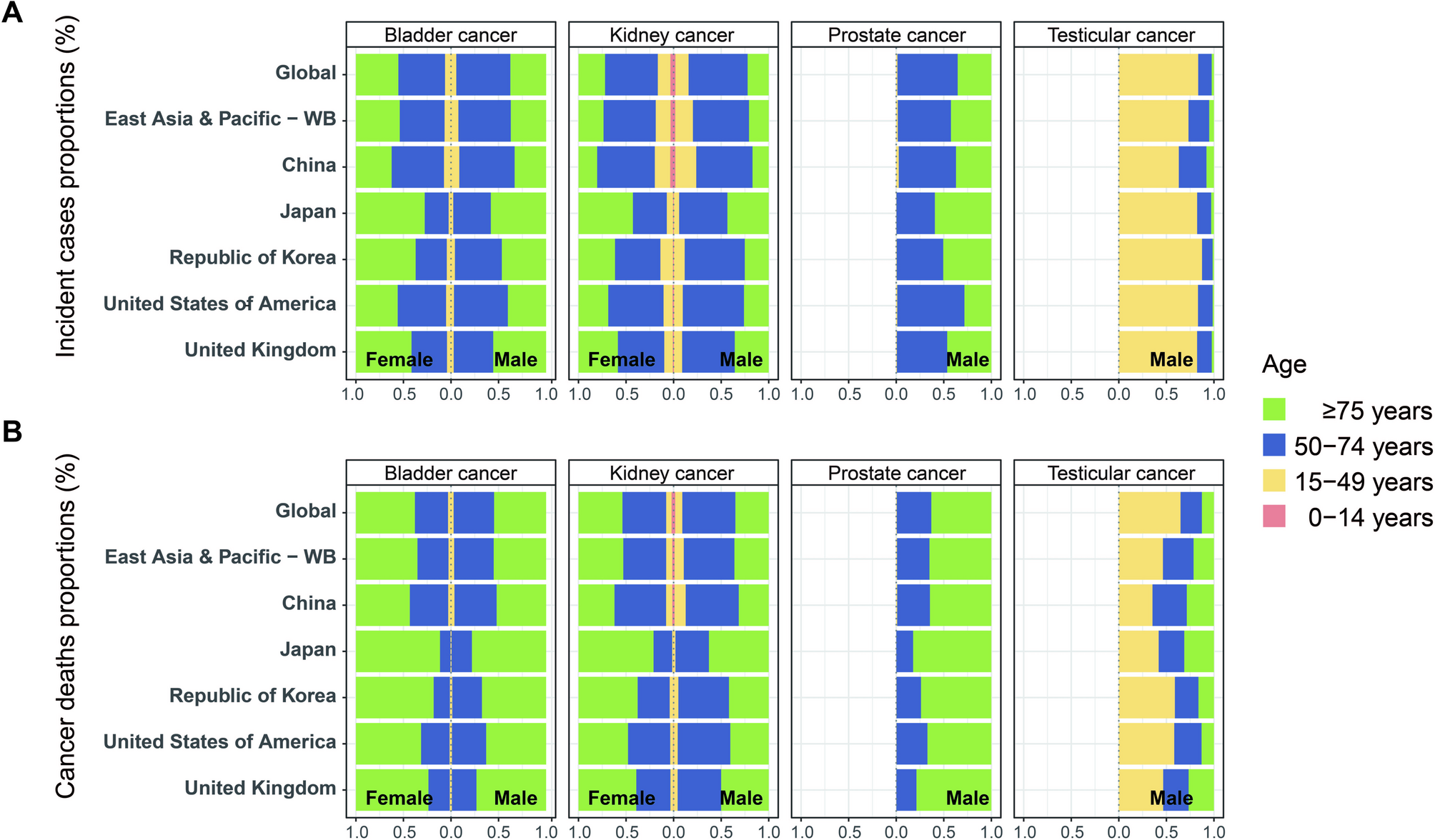
Table S1 shows the absolute number of incident cases of genitourinary cancers for four age groups in the global region, East Asia and Pacific region, China, Japan, the Republic of Korea, the US, and the UK. In 2021, China reported approximately 266,887 cases of genitourinary cancers, indicating a significant global and regional burden. Bladder, kidney, prostate, and testicular cancers in Chinese males represented 20.4%, 18.4%, 6.7%, and 7.3% of the global burden, respectively, and 65.4%, 63.1%, 38.5%, and 46.8% of the East Asia and Pacific region’s burden, respectively. Bladder and kidney cancer cases in Chinese females constituted 16.7% and 14.2% of the global cases, respectively, and 58.8% and 58.3% of East Asia and Pacific cases, respectively. Except for prostate and testicular cancers in males and bladder and kidney cancers in females, where case numbers in China were lower than those in the US, the overall number of genitourinary cancer cases in China exceeded those in other countries (Table S1). The distribution patterns across age groups in China for these cancers differed from those in Japan, the Republic of Korea, the US, and the UK (Table S1 and Fig. 1A). In China, both bladder and kidney cancers showed the greatest case numbers in the 50–74 age group, accounting for more than 50% of total cases across all age groups for both sexes. Prostate cancer in males also peaked in the same age range (50–74 years: 60.2%). Testicular cancer, on the other hand, had the highest incidence in the 15–49 age group (63.1%). The proportions of elderly patients (aged ≥ 75 years) with bladder, kidney, and prostate cancers in China were slightly lower than in other countries (all P-values < 0.05), whereas the proportion of elderly patients (aged ≥ 75 years) with testicular cancer was higher in China than in other countries (all P-values < 0.05, Table S1 and Fig. 1A).
Fig. 1
Age-specific proportions of incident and death cases of genitourinary cancers. (A) Proportions of incident cases by age group (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) for bladder, kidney, prostate, and testicular cancers across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK in GBD 2021. (B) Proportions of death cases by age group (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) for bladder, kidney, prostate, and testicular cancers across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK in GBD 2021
Table S2 presents age-stratified mortality data for genitourinary cancers across four age groups, including the global, the East Asia and Pacific, and selected countries (China, Japan, the Republic of Korea, the US, and the UK). In 2021, there were 108,589 deaths from bladder, kidney, prostate, and testicular cancers in China. Mortality among Chinese males constituted 21.5% (bladder cancer), 16.6% (kidney cancer), 8.6% (prostate cancer), and 10.9% (testicular cancer) of the global burden and 67.0%, 58.4%, 42.4%, and 55.0% of the East Asia and Pacific region’s burden, respectively. Bladder and kidney cancer deaths in females represented 17.0% and 13.2% of the global burden and 56.6% and 52.3% of the East Asia and Pacific burden, respectively. Except for prostate cancer, for which deaths in China were lower than those in the US, deaths from other genitourinary cancers in China were higher for both sexes (Table S2). The distribution of genitourinary cancer deaths in China (Table S2 and Fig. 1B) exhibited distinct age-specific patterns: bladder cancer deaths in both sexes (52.0% male; 56.7% female) and prostate cancer deaths in males (64.5%) peaked in the ≥ 75 years age group, whereas kidney cancer deaths in both sexes (55.8% male; 54.3% female) and testicular cancer deaths in males (36.1%) were most frequent in the 50–74 years age group. Notably, compared with other countries and regions included in our analysis, China had higher proportions of deaths before age 75 from bladder and kidney cancers in both sexes and prostate cancer in males (all P values < 0.05, Table S2, Fig. 1B).
Genitourinary cancer incidence and mortality ratesFor all age groups, except for the ASIR of male bladder cancer in China (90.53), which was slightly higher than thatin East Asia and Pacific (89.25), China’s ASIRs for genitourinary cancers in both sexes were generally lower than those in the global, East Asia and Pacific, Japan, the Republic of Korea, the US, and the UK (Tables 1 and 2). However, in specific age groups, China had the highest ASIRs for male kidney cancer in the 0–14 years age group (China 1.70 vs. global 1.24, East Asia and Pacific 1.41, Japan 0.70, the Republic of Korea 0.63, the US 1.33, and the UK 0.78) and for male testicular cancer in the ≥ 75 years age group (China 0.56 vs. global 0.54, East Asia and Pacific 0.47, Japan 0.27, the Republic of Korea 0.12, the US 0.50, and the UK 0.54) compared with the studied regions and countries (Table 1; Fig. 2A). Additionally, in the 15–49 years age group, China’s ASIRs for male bladder cancer (11.22), kidney cancer (15.37), and prostate cancer (3.61) exceeded those of Japan (bladder cancer: 9.95, kidney cancer: 11.62, prostate cancer: 3.04) and the Republic of Korea (bladder cancer: 8.38, kidney cancer: 12.06, prostate cancer: 2.39) (Table 1; Fig. 2A). For females, China’s ASIR for kidney cancer (1.50) in the 0–14 years age group was higher than that in Japan (1.04) and the Republic of Korea (0.64) (Table 2; Fig. 2A).
Table 1 The ASIRs and ASMRs of male bladder, kidney, prostate, and testicular cancers across ages and locations in 2021 (per 1,000,000)Table 2 The ASIRs and ASMRs of female bladder and kidney cancers across ages and locations in 2021 (per 1,000,000)Fig. 2
The ASIRs and ASMRs of genitourinary cancers by country and age groups. (A) The ASIRs of bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK in GBD 2021. (B) The ASMRs of bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK in GBD 2021. ASIRs, age-standardized incidence rates; ASMRs, age-standardized mortality rates
China’s ASMRs for the four genitourinary cancers were also generally lower than the global, East Asia and Pacific averages, as well as those in Japan, the Republic of Korea, the US, and the UK. However, several exceptions were observed (Tables 1 and 2). For example, China’s ASMR for male bladder cancer (43.19) was higher than those in East Asia and Pacific region (39.79), Japan (37.71), and the Republic of Korea (42.22). Additionally, China’s ASMR for male testicular cancer (1.52) was higher than that of Japan (1.23) and the Republic of Korea (0.43) (Table 1). China’s ASMR for female bladder cancer (9.19) was slightly higher than that in the Republic of Korea (8.82) (Table 2). Among the specific age groups, China had the highest ASMRs for male bladder cancer in the 15–49 years age group (China 1.94 vs. global 1.18, East Asia and Pacific 1.55, Japan 0.93, the Republic of Korea 0.81, US 1.08, and UK 1.51) and for male testicular cancer in the ≥ 75 years age group (China 0.38 vs. global 0.36, East Asia and Pacific 0.32, Japan 0.13, the Republic of Korea 0.05, the US 0.22, and the UK 0.26) compared with other regions and countries. Additionally, China’s ASMR for male kidney cancer in the 0–14 years age group was 0.35, which was lower than the global value of 0.47 but higher than those of Japan (0.11), the Republic of Korea (0.10), the US (0.16), and the UK (0.16) (Table 1; Fig. 2B). For female kidney cancer in the same age group (0–14 years), China’s ASMR was 0.23, which was lower than that of the global (0.32) and the UK (0.25) but higher than those of Japan (0.12), the Republic of Korea (0.08), and the US (0.20) (Table 2; Fig. 2B). Both male and female ASMRs for kidney cancer in China’s 0–14 years age group were comparable to those in East Asia and the Pacific’s level (Tables 1 and 2; Fig. 2B). For males aged 15–49 years, China’s ASMRs for kidney cancer (3.11) and prostate cancer (0.57) were higher than those in Japan (kidney cancer: 2.00, prostate cancer: 0.38) and the Republic of Korea (kidney cancer: 2.10, prostate cancer: 0.30) (Table 1; Fig. 2B).
China also had a relatively high incidence and mortality burden of bladder and kidney cancers in males. The male-to-female ratios of ASIRs and ASMRs for bladder cancer in the 15–49 and ≥ 75 years age groups and for kidney cancer across the 0–14, 15–49, and ≥ 75 years age groups were higher in China than in other countries and regions (Table S3). The MIRs for all genitourinary cancers in both sexes followed a similar pattern: they increased with age and peaked in the ≥ 75 years age group (Fig. 3A-B). In China, the MIRs for genitourinary cancers were generally similar to the global and East Asia and Pacific levels, except for lower MIRs for kidney cancer in children (0–14 years) and higher MIRs for bladder and prostate cancers in the elderly (≥ 75 years). Except for kidney cancer in both sexes in the ≥ 75 years age group and in male aged 50–74 years, where MIRs were lower than or equal to those in Japan, China’s MIRs for genitourinary cancers across all age groups were higher than those in Japan and the Republic of Korea. Compared with the US and the UK, China’s MIRs for bladder and kidney cancers in both sexes were similar to those in the UK but significantly higher than those in the US. Additionally, China had much higher MIRs for male prostate and testicular cancers across all age groups than the US and the UK (Fig. 3A-B).
Fig. 3
The MIRs of genitourinary cancers by countries and age groups. (A) The male MIRs of bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK in GBD 2021. (B) The female MIRs of bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK in GBD 2021. MIRs, mortality-to-incidence ratios
Trends in genitourinary cancer incidence and mortality ratesFrom 1990 to 2021, the ASIRs of genitourinary cancers exhibited varying trends across countries and regions (Fig. 4A-D and Table S4). For ASIRs of kidney cancer in the 0–14 years age group, an increasing trend was noted exclusively among Japanese females (AAPC of 0.87%), whereas globally and in East Asia and Pacific, as well as other countries, it either declined or stabilized from 1990 to 2021. In China, the historically high ASIRs of kidney cancer for both sexes aged 0–14 years decreased significantly (with AAPCs of -0.98% for males and − 2.73% for females). Despite this decline, China’s ASIRs for male kidney cancer in the 0–14 years age group remained above those of all other regions and countries. Moreover, China’s ASIR for female kidney cancer in the same age group (0–14 years) fell below those of Japan and the UK with rapid declines, yet was still higher than those of the US and the Republic of Korea (Fig. 4C-D and Table S4). In contrast, for the 15–49, 50–74, and ≥ 75 years age groups, kidney cancer ASIRs increased in most countries and regions, except for the US, which showed stable or declining trends in the 15–49 and 50–74 years age groups. Notably, in China, for males aged 15–49 years, the AAPC for kidney cancer was significantly higher (4.48% vs. global 1.34%, East Asia and Pacific 3.69%, Japan 1.19%, the Republic of Korea 3.72%, US 0%, and UK 1.48%), and thus the ASIR surpassed other regions and countries, ranking just behind two Western nations (Fig. 4A-B and Table S4). For bladder cancer, the ASIRs in the two Western countries had remained high over the past three decades, with a downward or stable trend observed across the age groups (15–49, 50–74, and ≥ 75 years) in the UK, in contrast with a slight upward trend in both sexes aged ≥ 75 years and females aged 15–49 years and ≥ 75 years in the US. Although the ASIRs of bladder cancer in East Asia and Pacific and three Asian countries were relatively lower from 1990 to 2021, the increasing trends in male ASIRs were pronounced, with the AAPCs in the three Asian countries much higher than those in Western nations across the same age groups (15–49, 50–74, ≥ 75 years). Notably, the incidence rate among Chinese males aged 15–49 showed an accelerated increase (AAPC of 2.14%) compared with the global of 0.41%, East Asia and Pacific of 1.70%, Japan of 0.58%, the Republic of Korea of 1.04%, the US of 0.33%, and the UK of -0.66%, leading China’s ASIR to rank second only to the US (Fig. 4A-D and Table S4). For prostate cancer, with the exception of the US in the 50–74 years age group, as well as in those aged ≥ 75 years in the global, the US and the UK, all other studied regions and countries showed increasing trends of ASIRs across all age groups (15–49, 50–74, and ≥ 75 years) from 1990 to 2021. Notably, East Asia and Pacific regions showed a more pronounced increase in prostate cancer incidence, with the Republic of Korea leading in AAPCs, followed by China and Japan across all age groups (15–49, 50–74, and ≥ 75 years) (Fig. 4A-B and Table S4). For testicular cancer, the two Western nations maintained higher incidence rates than other countries and regions. In contrast to the UK and Japan, which experienced declining or stable ASIRs during the study period, China and the Republic of Korea showed increasing trends with higher AAPCs. Despite starting from the lower rates, China’s ASIRs of testicular cancer have risen to be the highest among countries in the ≥ 75 years age group, with an AAPC of 1.43% (Fig. 4A-B and Table S4).
Fig. 4
Trends in annual ASIRs of genitourinary cancers from 1990 to 2021. (A) Temporal trends in ASIRs of male bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK from 1990 to 2021. (B) AAPCs in the ASIRs of male bladder, kidney, prostate, and testicular cancers across age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK). (C) Temporal trends in ASIRs of female bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK from 1990 to 2021. (D) AAPCs in the ASIRs of female bladder, kidney, prostate, and testicular cancers across age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK). AAPCs, average annual percent changes; ASIRs, age-standardized incidence rates
Notable differences in ASMRs trends were observed between Asian and Western nations from 1990 to 2021 (Fig. 5A-D and Table S4). For kidney cancer, all studied regions and countries exhibited significant decreases in ASMRs for both sexes aged 0–14 years, with China experiencing the largest decrease (an AAPC of -3.33% for males and − 5.30% for females). Except for Japan, Asian countries reported an increasing trend in ASMRs of kidney cancer for males aged 15–49 and 50–74 years, which contrasted with the decreasing and stable trends in Western countries. Notably, China’s rapidly increasing rates (AAPC: 2.13%) of kidney cancer mortality in males aged 15–49 caused the trend line to steeply increase, surpassing both Japan and the Republic of Korea and approaching the levels of the US. In the ≥ 75 years age group, all regions and countries, with the exception of China in terms of female kidney cancer, experienced significantly increasing trends in ASMRs for both sexes (Fig. 5A-D and Table S4). For bladder cancer, increasing trends in ASMRs were observed for females aged 15–49 years (with an AAPC of 1.02%) and both sexes aged ≥ 75 years (with AAPCs of 0.44% for males and 0.92% for females) in Japan, whereas other regions and countries showed declining or stable trends. Despite a downward trend, China’s bladder cancer mortality in the 15–49 years male group remained higher than that in other countries (Fig. 5A-D and Table S4). For prostate cancer, mortality in Western countries exceeded those in the global and Asian countries, yet the Western countries displayed general decline or stable trends, whereas East Asia and pacific region showed a marked upturn in mortality across all age groups. Among Asians countries studied, China’s 15–49 years age group showed increasing trends, leading to higher mortality rates than those of Japan and the Republic of Korea, which showed stable trends similar to those of Western countries (Fig. 5A-B and Table S4). Testicular tumor mortality trended downward in all countries and regions across all age groups; however, in China’s ≥ 75 years age group, the fluctuating mortality rates masked a higher mortality rate than those in Japan, the Republic of Korea, and Western countries (Fig. 5A-B and Table S4).
Fig. 5
Trends in annual ASMRs of genitourinary cancers from 1990 to 2021. (A) Temporal trends in ASMRs of male bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK from 1990 to 2021. (B) AAPCs in the ASMRs of male bladder, kidney, prostate, and testicular cancers across age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK). (C) Temporal trends in ASMRs of female bladder, kidney, prostate, and testicular cancers for four age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) across global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK from 1990 to 2021. (D) AAPCs in the ASMRs of female bladder, kidney, prostate, and testicular cancers across age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK). AAPCs, average annual percent changes; ASMRs, age-standardized mortality rates
China experienced a significant widening of sex differences in both bladder and kidney cancers in terms of incidence and mortality across all age groups. The trends in the male-to-female ratios for incidence (ASIRs) and mortality (ASMRs) increased and were higher than those in other countries and regions, particularly in the 15–49 and ≥ 75 years age groups for bladder cancer and in the 0–14, 15–49, and ≥ 75 years age groups for kidney cancer (Fig. 6A-B). Regarding the trends in the MIRs (Fig. 7A-D), despite the generally decreasing trends observed in China and other countries and regions, China still presented higher MIRs for genitourinary cancers, especially in the 50–74 and ≥ 75 years age groups for male bladder cancer and for prostate cancer and in the 15–49, 50–74, and ≥ 75 years age groups for testicular cancer.
Fig. 6
Trends of male-to-female ratios of ASIRs and ASMRs in bladder and kidney cancers. (A) Trends of male-to-female ratios in bladder cancer incidence and mortality rates across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (B) Trends of male-to-female ratios in kidney cancer incidence and mortality rates across age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021
Fig. 7
Trends of MIRs in genitourinary cancers across sexes, locations, and ages from 1990 to 2021. (A) Trends of MIRs in bladder cancer across sexes (male and female), age groups (15–49 years, 50–74 years and ≥ 75 years), and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (B) Trends of MIRs in kidney cancer across sexes (male and female), age groups (0–14 years, 15–49 years, 50–74 years and ≥ 75 years), and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (C) Trends of MIRs in prostate cancer across age groups (15–49 years, 50–74 years and ≥ 75 years), and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (D) Trends of MIRs in testicular cancer across age groups (15–49 years, 50–74 years and ≥ 75 years), and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. MIRs, mortality to incidence ratios
Decomposition analysisThe decomposition analysis revealed that the increase in incident cases of genitourinary cancers in most regions and countries from 1990 to 2021 was attributable to aging, population growth, and epidemiological changes, which collectively contributed to a growing burden of these cancers over time (Fig. 8A-F and Table S5).
Fig. 8
Decomposition analysis on changes in genitourinary cancers incidence and mortality across sexes and locations from 1990 to 2021. Absolute changes and contribution proportions of (A) male kidney cancer incidence, (B) male bladder cancer incidence, (C) male prostate cancer incidence, (D) male testicular cancer incidence, (E) female kidney cancer incidence, and (F) female bladder cancer incidence attributed to the three factors (aging, population growth, and epidemiological change). Absolute changes and contribution proportions of (G) male kidney cancer mortality, (H) male bladder cancer mortality, (I) male prostate cancer mortality, (J) male testicular cancer mortality, (K) female kidney cancer mortality, and (L) female bladder cancer mortality attributed to the three factors (aging, population growth, and epidemiological change). The black dot in A-L represents the combined effect of all three factors, including aging, population growth, and epidemiological change
Globally, population growth was the primary driver of the increase in the incidence of genitourinary cancers (bladder cancer: males 64.41%, females 76.89%; kidney cancer: males 40.12%, females 51.93%; prostate cancer: 50.61%; and testicular cancer: 57.06%, Fig. 8A-F and Table S5). In East Asia and Pacific, aging was the main positive driver for the increase in the incidence of bladder cancer in both males (48.47%) and females (66.03%), as well as for prostate cancer (40.06%) and female kidney cancer (39.23%), whereas epidemiological changes primarily affect the increase in incidence of male kidney cancer (48.18%) and testicular cancer (67.27%, Fig. 8A-F and Table S5). In three Asian countries, aging made the greatest contribution to the increase in the incidence of bladder cancer in both males and females, with contributions of 51.80% in men and 81.58% in women in China, 69.03% in men and 68.69% in women in Japan, and 64.90% in men and 66.78% in women in the Republic of Korea (Fig. 8A and E, and Table S5). In China (males 55.94% and females 42.18%) and the Republic of Korea (males 46.08% and females 47.33%), the increase in the incidence of male and female kidney cancer was also largely due to epidemiological changes, whereas in Japan, aging was the main factor (males 55.81% and females 52.04%, Fig. 8B and F, and Table S5). The increase in male prostate and testicular cancer incidence was driven predominantly by epidemiological changes in China (44.44% and 76.45%), Japan (49.67% and 361.74%), and the Republic of Korea (47.42% and 95.75%, Fig. 8C-D and Table S5). In the US, the increase in the incidence of male bladder (51.14%), kidney (51.67%), and prostate (79.33%) cancers was driven mainly by aging, with testicular cancer being strongly influenced by epidemiological changes (62.84%) and female bladder (60.22%) and kidney (55.72%) cancers caused by population growth (Fig. 8A-F and Table S5). The UK observed an increase in the incidence of kidney cancer, which was driven primarily by contributions from epidemiological changes in both males (41.40%) and females (59.29%). Aging exerted a substantial positive influence on the increase in the incidence of male bladder (1115.72%) and prostate (41.21%) cancers, while population growth was the main driver of female bladder (208.87%) cancers (Fig. 8A-F and Table S5).
According to the decomposition analysis, population growth was the major positive driver for the increases in mortality from bladder cancer in males (80.64%) and females (95.14%), prostate cancer (69.06%) and testicular cancer (122.34%) in males, and kidney cancer (64.26%) in females globally (Fig. 8G-L and Table S6). Population growth also primarily impacted the increase in testicular cancer mortality in East Asia and Pacific (114.39%), China (170.14%), and the US (183.11%), as well as for female bladder cancer in the US (69.67%) and the UK (206.07%), and for female kidney cancer in the US (74.30%, Fig. 8J-L and Table S6). Aging was the main positive driver of increased bladder cancer mortality in males in East Asia and Pacific (76.75%), China (94.78%), Japan (80.26%), the Republic of Korea (109.74%), the US (56.21%), and the UK (526.60%, Fig. 8G and Table S6). Male kidney cancer (global 48.54%, East Asia and Pacific 53.09%, China 55.55%, Japan 70.58%, Republic of Korea 66.94%, the US 72.57%, and the UK 53.82%, Fig. 8H and Table S6) and prostate cancer (global 57.85%, East Asia and Pacific 60.10%, China 64.95%, Japan 69.00%, Republic of Korea 61.49%, the US 242.29%, and the UK 110.48%, Fig. 8I and Table S6) in all studied regions and countries, as well as female bladder and kidney cancer in East Asia and Pacific (106.24% and 63.87%) and three Asian countries (bladder cancer: China 186.66%, Japan 72.23%, and the Republic of Korea 101.96%; kidney cancer: China 79.60%, Japan 63.75%, and the Republic of Korea 67.82%) were also predominantly driven by aging (Fig. 8K-L and Table S6). Although epidemiological changes contributed positively to the increased mortality of male kidney and prostate cancers, as well as female kidney cancers in Asian regions and countries, they generally contributed negatively to the overall mortality burden of all genitourinary cancers in Western countries (Fig. 8G-L and Table S6). This negative impact was particularly pronounced for testicular cancer mortality (Fig. 8J and Table S6), where the negative contributions of epidemiological changes surpassed the positive increases attributed to population growth and aging, resulting in the observed decreases in the numbers of testicular cancer-related deaths in Japan (-38), the Republic of Korea (-10), and the UK (-101).
Risk factor trendsThe GBD did not provide risk factors for testicular cancer mortality. Therefore, in our study, we analyzed the impacts of smoking, a common modifiable risk factor, on kidney, bladder, and prostate cancers (Fig. 9A-B and Figure S1A-C). Additionally, we investigated the effects of a high FPG level on bladder cancer (Fig. 9C-D and Figure S2) and a high BMI on kidney cancer (Fig. 9E-F and Figure S3). Among these cancers, bladder cancer consistently recorded the highest PAFs for smoking-related mortality across all age groups and for both sexes. Notably, Chinese males showed an increase in PAFs for kidney, bladder, and prostate cancers, which contrasts with the general downward trend observed in other countries. Moreover, China continues to exhibit significantly higher PAFs for smoking-related mortality in male genitourinary cancers (Fig. 9A-B). For high FPG, an overall increasing trend in PAFs was observed for bladder cancer mortality in the 15–49 years age group in both sexes in China (Fig. 9C-D). Furthermore, a high BMI was identified as another major risk factor for kidney cancer mortality in China, with increasing trends observed across all age groups and for both sexes. China’s PAFs of high BMI-related kidney cancer mortality were second only to those globally, the US, and the UK (Fig. 9E-F).
Fig. 9
PAFs of genitourinary cancers mortality due to risk factors across sexes, locations, and ages from 1990 to 2021. (A) PAFs of smoking-related mortality for male kidney, bladder, and prostate cancers across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (B) PAFs of smoking-related mortality for female kidney, bladder, and prostate cancers across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (C) PAFs of high FPG-related mortality for male bladder cancer across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (D) PAFs of high FPG-related mortality for female bladder cancer across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (E) PAFs of high BMI-related mortality for male kidney cancer across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. (F) PAFs of high BMI-related mortality for female kidney cancer across age groups (15–49 years, 50–74 years and ≥ 75 years) and geographic locations (global, East Asia and Pacific, China, Japan, the Republic of Korea, the US and the UK) from 1990 to 2021. BMI, body mass index; FPG, fasting plasma glucose; PAFs, population-attributable fractions
The attributable numbers of kidney, bladder, and prostate cancer-related deaths due to smoking are displayed in Figure S1A-C. Smoking-related mortality was more common in the 50–74 and ≥ 75 years age groups. Other than the 15–49 and 50–74 years age groups, increasing trends in attributable numbers of male kidney, bladder, and prostate cancer mortality related to smoking were observed in the ≥ 75 years age group globally, in the East Asia and Pacific, and in the three Asian countries, with the highest increase in attributable numbers for bladder cancer. Compared with other countries, China exhibited a distinct upward trend in smoking-attributable mortality for these cancers in the 50–74 years age group. Although China displayed similar trends in mortality attributable to a high FPG and a high BMI as other countries (Figure S2 and Figure S3), the attributable numbers for bladder cancer mortality related to high FPG remained consistently greater across all age groups and for both sexes.
Comments (0)