
Remember me
Patient centricity is an essential concept in pharmaceutical research and development, extending beyond participation in clinical trials, throughout the lifecycle of a medicinal product [1,2,3,4,5,6]. Patients’ experiences of living with their disease and their unmet needs appropriately shape the balance of benefits versus risks associated with treatments [3, 4, 7,8,9,10]. In pre-clinical and early clinical phases of drug development, patients can provide significant insights into unmet medical needs, research priorities and endpoints, study design, and patient priorities [3, 11,12,13,14,15]. Integrating patients’ perspectives in clinical development increases the likelihood of successful safety monitoring and compliance. In Phase II–III studies, patients’ perspective can be considered to inform the safety guidance for clinical trials and their ethical review, thresholds for pausing or stopping studies, and the appropriate endpoints for regulatory approval. Furthermore, patients can review risk minimization documents to be used in drug development (e.g., safety aspects of the informed consent forms) and support the preparation of post-marketing educational programs. Once medicines are approved, patients’ lived experiences provide real-world evidence of longer-term effectiveness and safety [11, 12, 14, 16,17,18,19]. The post-marketing lifecycle management period is generally the time when rare events can emerge with broader and long-term use of medicines. Patients’ insights around these events and the appropriate communication of safety updates are natural and much-needed extensions of patient engagement (PE) in the ongoing safe use of medicines.
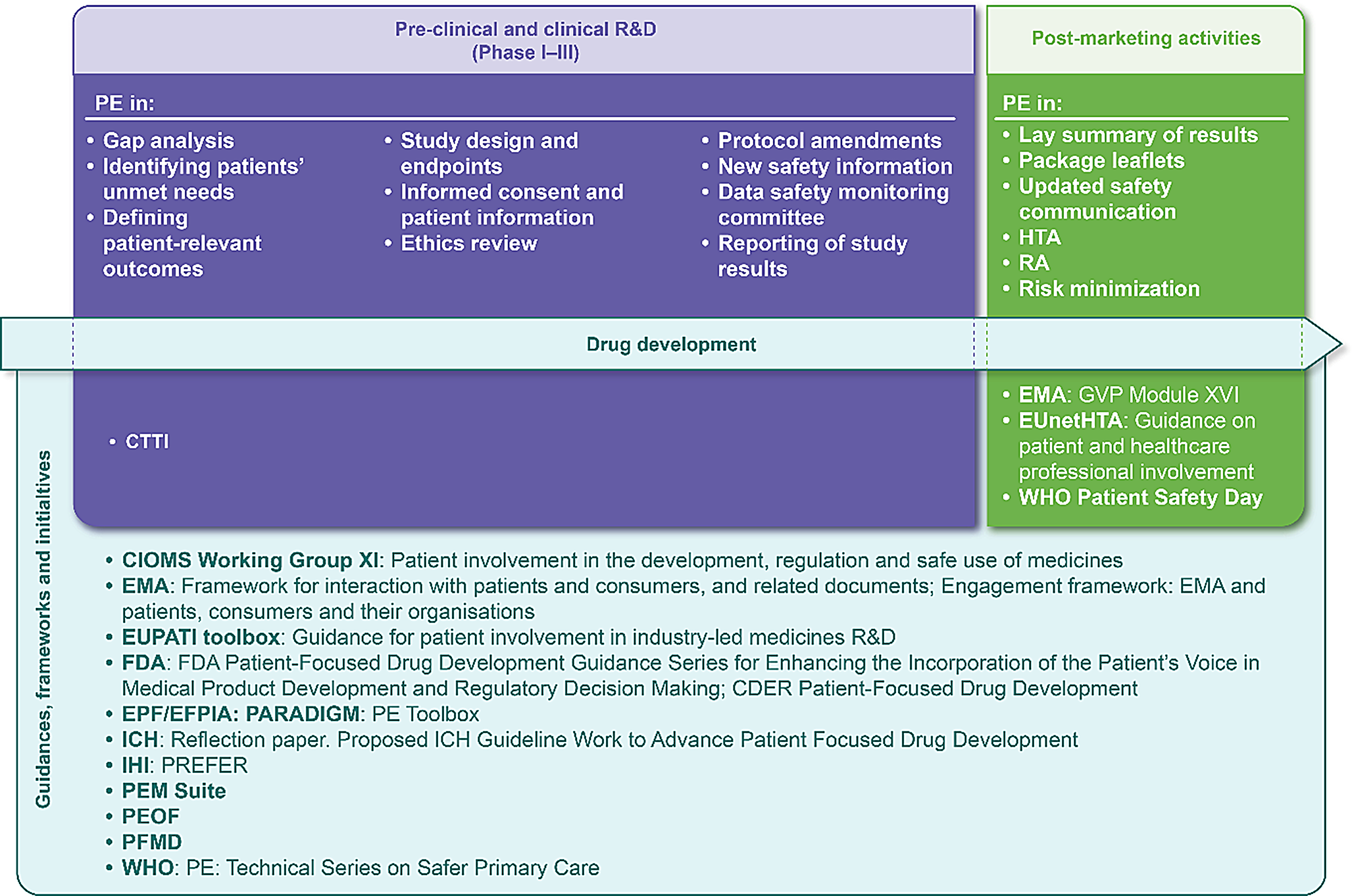
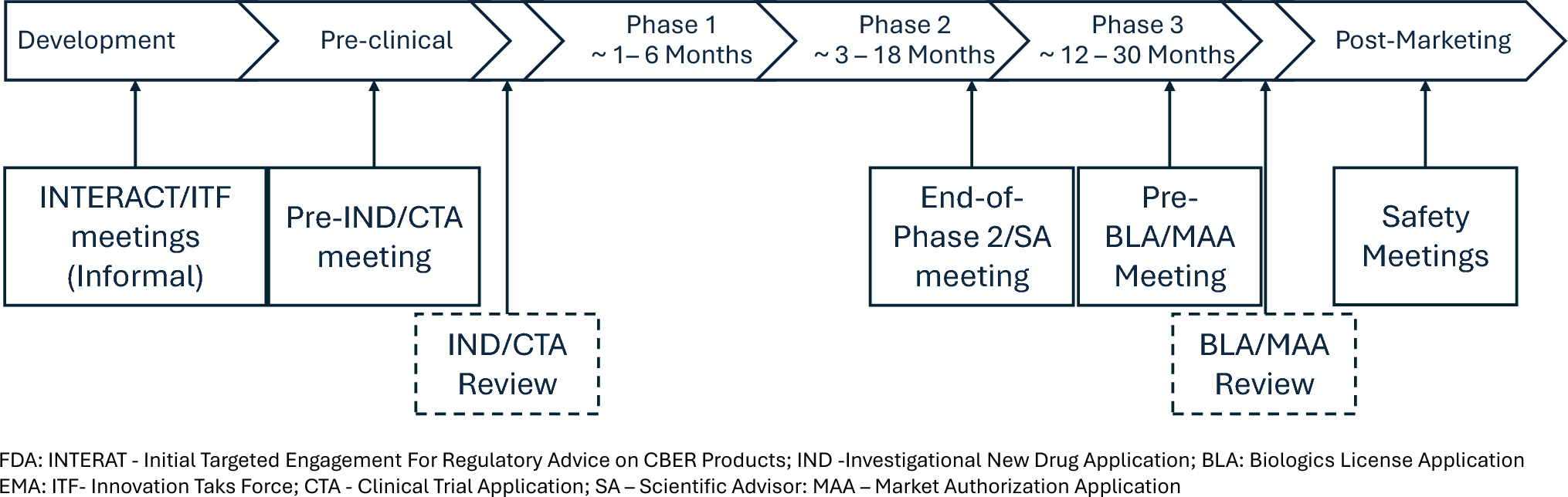
Various initiatives have been launched to involve patients across the product lifecycle, with regulatory authorities increasingly integrating the patient’s voice into their policies and recommendations (Fig. 1) [11, 19,20,21,22,23,24,25,26,27,28,29,30,31,32]. These initiatives consider some of the challenges of PE during drug development [11, 16,17,18,19, 33], which are also germane in post-marketing phase, such as:
Fig. 1
Drug development timeline with key areas of PE and the main guidances, frameworks and initiatives (non-exhaustive) integrating PE across the product lifecycle. CIOMS, Council for International Organizations of Medical Sciences; CDER, Center for Drug Evaluation and Research; CTTI, Clinical Trials Transformation Initiative; EFPIA, European Federation of Pharmaceutical Industries and Associations; EMA, European Medicines Agency; EPF, European Patient Forum; EUnetHTA, European network for Health Technology Assessment; EUPATI, European Patients’ Academy on Therapeutic Innovation; FDA, Food and Drug Administration; GVP, good pharmacovigilance practices; HTA, Health Technology Assessment; ICH, International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use; IHI, Innovative Health Initiative; PARADIGM, Patients Active in Research and Dialogues for an Improved Generation of Medicines; PE, patient engagement; PEM, Patient Engagement Management; PEOF, Patient Engagement Open Forum; PFMD, Patient-Focused Medicines Development; PREFER, Patient Preferences in benefit risk assessments during the drug life cycle; RA, Regulatory Affairs; R&D, Research and Development; WHO, World Health Organization
Communicating in patient-friendly but not condescending language.
Inclusion of representative patients and patient organizations (POs) to provide informative perspectives for the patient populations of interest, including surrogates for patients who are very young, non-verbal, cognitively impaired, or otherwise in need of representation by an appropriate ally.
Use of emerging technologies to provide broader access to medicines and communications without excluding populations who may already be underserved.
Alliance with POs to support patients’ needs without overburdening the organizations.
Support for patient participation that recognizes the value of their time and contribution without coercing their involvement.
Conceptual frameworks and roadmaps providing guidance on patient centricity in pharmaceutical research have been published to facilitate consistent PE [3, 4, 15, 34,35,36,37,38,39,40]. These frameworks and roadmaps have extended to support PE in pharmacovigilance [40,41,42,43]. One such roadmap describes a pragmatic approach for pharmacovigilance departments within the pharmaceutical industry, highlighting three hallmarks crucial for patient-centered safety departments: (1) adoption of a company-wide patient-centered culture supported by governance structure and ongoing training; (2) development of a PE framework, both internally and externally, through promoting PE with patient communities; (3) acquiring patient-centered competencies, such as increasing patient access to understandable information, e.g., labelling and other patient-targeted pharmacovigilance materials [43]. Additionally, the International Society of Pharmacovigilance has recently established the PE Special Interest Group to develop and promote PE in pharmacovigilance through various research and training activities, as well as publications, to raise awareness of the importance of PE in safety in collaboration with patients and POs, regulatory authorities, and other relevant stakeholders [40]. Various regulatory guidances exist to support the incorporation of the patient’s perspective specifically into pharmacovigilance activities (Table 1).
Table 1 Examples of key initiatives and guidances incorporating patient voice in pharmaceutical drug safety and pharmacovigilanceRegarding risk management, the recently effective European Medicines Agency (EMA) guideline on good pharmacovigilance practices (GVP) Module XVI (Revision 3) [44] and the United States (US) Food and Drug Administration (FDA) risk evaluation and mitigation strategy (REMS) draft Logic Model [45] have further reinforced the importance of patient-centered healthcare involving various stakeholders (including patients) to create effective risk minimization strategies. These guidelines describe the opportunity to engage with patients across all stages of risk minimization design, implementation, and evaluation, to support appropriate adoption and maintenance of the risk minimization recommendations in medical practice.
While the guidelines re-affirm the importance of PE in risk management, to our knowledge, frameworks supporting the systematic adoption of PE by Marketing Authorization Holders (MAHs) across the risk management system are limited. Furthermore, there is limited guidance to support balancing value with timely PE in pharmacovigilance deliverables across the product lifecycle. Thus, PE may occur ad hoc and in a reactive manner, and in some instances be considered merely symbolic or tokenistic [46], with limited impact on the effectiveness of the risk management activities. Assessing the impact of PE in risk minimization activities is likewise challenging due to this lack of a systematic approach for such engagement and the limited published data describing PE outcomes. According to the available literature, to date, only one study reported proposals for engaging patients in risk minimization; this study revealed gaps in stakeholder input and research related to critical elements of implementation of risk minimization measures (RMMs), and indicated the need for an improved PE in RMM decision making [41]. However, to date, there is no study published on the impact of patient review of RMM materials.
To support MAHs to leverage a systematic and practical approach for PE across the pharmacovigilance system, including risk management, we propose a framework for consideration and adaptation according to company-specific needs. A plain language summary describing this framework is shown in Fig. 2.
Fig. 2
Comments (0)