Data Source
We used data from the JMDC claims database, which has been previously described in detail [15]. Briefly, the JMDC claims database is a large-scale database containing medical claims of large- and medium-sized company employees and their dependent family members aged < 75 years. Since 2005, the number of individuals in the JMDC database has increased consistently, reaching a cumulative total of more than 20 million by the end of 2024. The JMDC database includes all the monthly claims for outpatient and inpatient diagnoses and procedures, prescriptions, and dispensations of drugs recorded as the Japanese original drug codes and product names, and the World Health Organization Anatomical Therapeutic Chemical (ATC) classification [16]. In addition, the data included the anonymized IDs of medical institutions, with which we could discern which drug was prescribed by the medical institution, as well as the type of medical institution: clinics (defined in Japan as medical institutions with no or < 20 beds for hospitalization), university-related hospitals, public hospitals, and other hospitals (including private hospitals receiving reimbursement from the health insurance system in Japan). We employed the most recent dataset, extracted in November 2024, which included data from January 2005 to May 2024. The data used in this study were anonymized and processed anonymously by JMDC, Inc.
For comparison, we also used the National Database (NDB) Open Data of Health Insurance Claims from April 2022 to March 2023, which is a summary table of the total use of drugs compiled by the government [17] and covers all Japanese citizens except those living with public financial assistance.
This study was approved by the Ethics Committees of the University of Tsukuba, Ibaraki, Japan (approval number 2099) and Meiji Pharmaceutical University, Tokyo, Japan (approval number 202462). The analyses were conducted independently at each study location to verify and obtain similar results.
Study Population
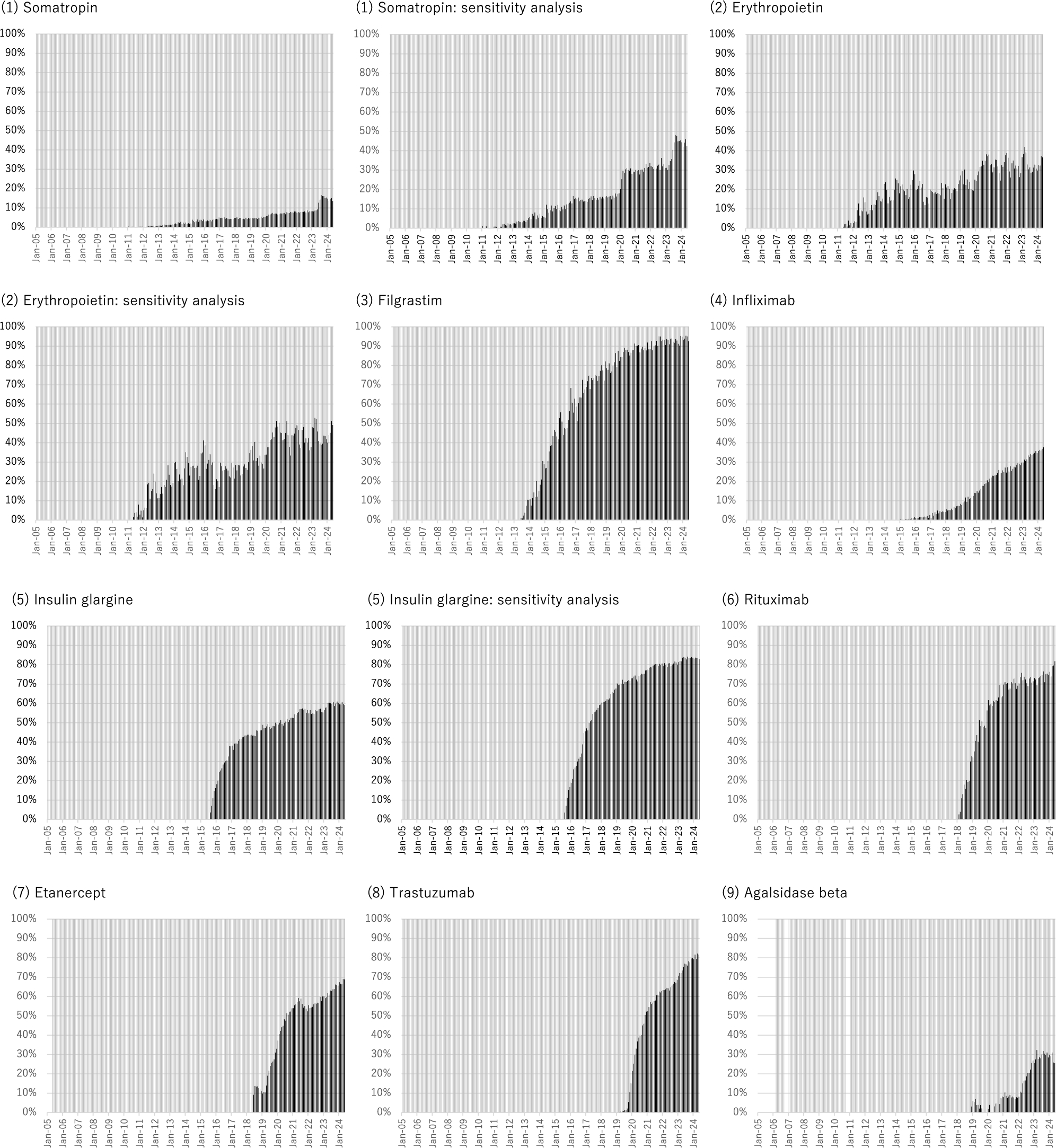
We identified patients receiving at least one prescription of all 17 biologics (for which biosimilars were approved and marketed by 2024) available in Japan during the study period, including somatropin, erythropoietin (including both epoetin alfa and epoetin beta), filgrastim, infliximab, insulin glargine, rituximab, etanercept, trastuzumab, agalsidase beta, bevacizumab, darbepoetin alfa, teriparatide, insulin lispro, adalimumab, insulin aspart, ranibizumab, and pegfilgrastim. For each of the 17 biologics, we created a list of product names (based on at least one prescription record in the JMDC database during the study period) using the ATC classification system, classifying them as original biologics or biosimilars (Supplementary Table S1). In the main analysis, we included all these biologics for our analysis. However, for several biologics (somatropin, erythropoietin, insulin glargine, darbepoetin alfa, insulin lispro, and insulin aspart), the original biologics other than the reference product of the biosimilar were approved (Supplementary Table S1). Thus, in the sensitivity analysis, we restricted the analysis to biosimilars and their reference products. In addition, there is one authorized generic (AG) biologic drug for darbepoetin alfa in Japan, which does not have a brand name on its label but is composed of the same drug component as the original biologics [18]. We included this AG biological drug in the biosimilars in the main analysis, but excluded it from our sensitivity analysis.
Data Analysis
After summarizing the demographics (age and sex) of the study population by biologics, we estimated and illustrated the monthly trends in the proportion of prescriptions of original biologics and biosimilars (among the total prescriptions for each biologic) from January 2005 to May 2024. In addition, we compared the statistics (i.e., the number and proportion of biosimilars among the total prescriptions for each biologic) in the JMDC database with those estimated from the NDB Open Data of Health Insurance Claims from April 2022 to March 2023 [17].
Next, at the individual level, we estimated the proportions of (i) patients receiving original biologics only, (ii) those receiving biosimilars only, (iii) those switching from original biologics to biosimilars, (iv) those switching from biosimilars to original biologics, and (v) unknown (because both original biologics and biosimilars were prescribed in the same month, we could not determine which was prescribed earlier from the monthly claims alone) during the study period from January 2005 to May 2024 in the main analysis. Additionally, we restricted the period of the analysis from the time each biosimilar entered the Japanese market to May 2024.
Finally, at the institutional level, among medical institutions with at least one prescription of original biologics, we estimated the proportion of medical institutions starting the prescription of biosimilars during the study period by the type of medical institution (clinics, university-related hospitals, public hospitals, and other hospitals) and 17 biologics.
An additional analysis was carried out restricted to patients who visit medical institutions introducing biosimilars during the study period. In the same way as the main analysis, the proportions of (i) patients receiving original biologics only, (ii) those receiving biosimilars only, (iii) those switching from original biologics to biosimilars, (iv) those switching from biosimilars to original biologics, and (v) unknown, during the study period (from January 2005 to May 2024) and from the time each biosimilar entered the Japanese market to May 2024 were estimated.
All the analyses were performed using STATA version 17 software (StataCorp, College Station, TX, USA).

Comments (0)