This study provides a comprehensive analysis of the spatial accessibility of radiation oncology and radiotherapy services in Germany. Information about the anticipated capacities allowed us to visualize regional shortages as well as vulnerability of ROC services. The methodology of systematically investigating the redistribution of catchment areas and capacities (ReDNA) used in this manuscript is unique and has never been described for radiation oncology or other medical specialties before. The methodology allows one to stress-test the national supply of RT services for local ROC failure. It appears to be generalizable to other countries or specialties and easily allows the addition of additional information, if available.
Spatial accessibility
Several groups have investigated the accessibility of ROCs. The concept of accessibility includes limitations to access due to economic, social, or institutional barriers. Many of these barriers do not apply to Germany, as the general social insurance system covers not only the treatment costs, but also transportation. Hence, in Germany, the spatial accessibility largely equals the accessibility of ROCs.
A recently published systematic review of 168 publications described an expected high heterogeneity, depending primarily on the economic background and the degree of urbanization of the region under study. Accordingly, mean travel distances in urban regions in the US ranged between 9.26 and 16 miles (14.9–25.7 km), while distances in rural areas were significantly longer (40.2–59 miles, 64.7–95 km) [33]. Furthermore, travel distances are an important factor in calculating the environmental impact of RT, as recently shown in an extensive life cycle analysis of four large academic centers in the US [34].
The locations of ROCs are distributed in relation to resident density. Hence, metropolitan regions offer a high density of ROC options to their residents, allowing free choice of the treating ROC with minimal additional effort. On the other hand, residents of rural regions or federal states with a high proportion of rural regions are more likely to be treated at the closest ROC, as the effort to reach competing ROCs might be too large. Importantly, Germany allows treatment in any ROC, not restricting patients to their federal state or residence.
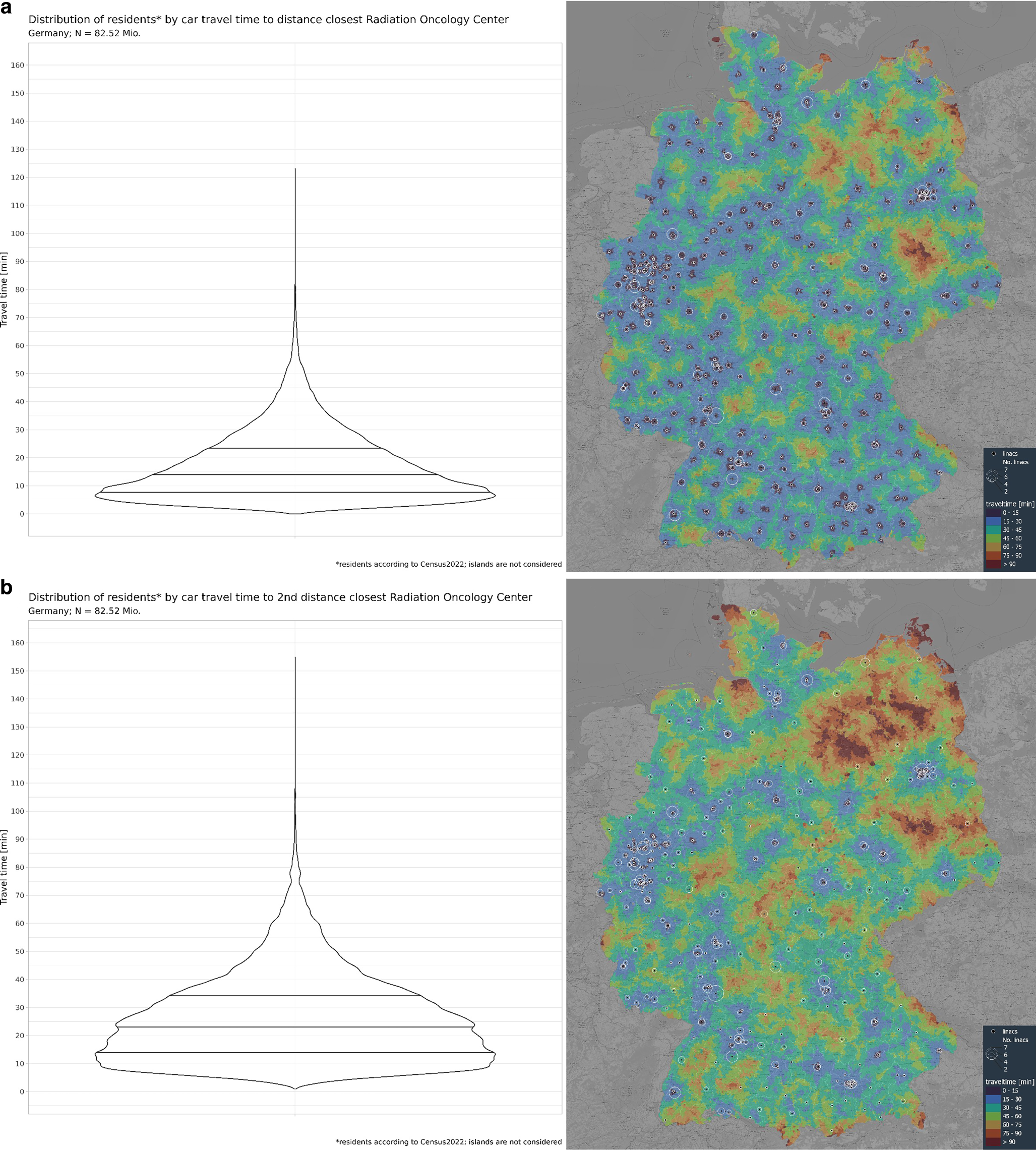
With regard to the German oncologic infrastructure, the available literature is sparse. An article from 2021 investigated the spatial accessibility to specialist breast cancer treatment in Bavaria. The article reported a mean travel time of 13 min (0–73 min) in urban and 21 min (0–79 min) in rural areas [35]. Furthermore, a recent article investigated the real-life catchment area of four ROCs based on real data from 4198 treated breast cancer patients. The average travel distance was 37.2 km per fraction or 18.6 km per single trip. These results fit well with our data, with mean distances of 15.5 km (distance closest ROC) and 16.7 km (time-closest ROC), especially as patients might chose the second- or third-closest ROC due to personal decisions [36]. Considering a wide range of travel times and distances in an international context, Germany provides one of the narrowest networks of RT services worldwide [33]. With as few as 238,185 inhabitants per ROC in Germany (4.2 ROC per million), only Switzerland has a higher density of ROCs in Europe (4.7 ROCs per million inhabitants) [22]. With 1.9 linacs per ROC, the size of German ROCs is below the European average (median 2.6), only Bulgaria (0.9), Belarus (1.5), and Switzerland (1.6) have fewer Linacs per ROC [22].
Investigating travelling times to the second- or third-closest or more distant ROC allows the accessibility of a second opinion to be investigated for the first time. We describe important differences in the difficulties of finding a second specialist especially in rural regions, while inhabitants of metropolitan regions can choose between several ROCs with only negligible travel distances. Especially carless inhabitants in rural regions are disproportionately impacted by extended travel times when the nearest ROC is unavailable. As the proportion of inhabitants per ROC is almost equal in between urban and rural regions, larger travel distances are an inevitable consequence of the uneven distribution of the population. Whether this is associated with an effect on outcomes is unknown.
Vulnerability
The current work is the first investigation not only for the closest facility but also for the second to each subsequently next ROC. This enabled us to stress-test the national ROC infrastructure by investigating the effect of local ROC failure on the spatial accessibility and workload of the remaining ROCs. This allows us to quantify the local vulnerability of the radiation oncology supply. Thereby, we identified regions with a relevant vulnerability to local incidences affecting ROCs. Modeling ROC capacities by regional networks enhances the robustness of this approach.
Another common method to investigate catchment areas is the “two-step floating catchment area method” [37]. This methodology allows one to incorporate multiple additional information, although it is not designed to model elimination of centers and subsequently re-evaluate the accessibility. The “three-step floating catchment area” is designed to overcome this limitation, however, it is usually applied only at the level of cities or limited regions [38]. Furthermore, the demand for services decays in predefined travel-time levels, which inadequately reflects the demand for treatment of acute life-threatening diseases, such as cancer.
In the absence of more detailed information on structural and personal infrastructure, our proposed methodology provides the most accurate approximation for estimating ROC supply and its vulnerability. Surprisingly, there is no research on this topic available. Related work investigates the search for the most-effective localization of new facilities. A landmark study from Brazil proposed a shortage index based on regional incidences and ROC supply. This approach is a suitable approach to deal with severe undersupply and provides information on potential oversupply. A shortcoming is the lack of accessibility information, as only regions and states were used as a basis for the score [39].
In summary, our data show a high level of resilience in most regions of Germany, yet at the cost of a significant increase in travel times of up to an additional 19.6 min (inhabitants of cities in rural regions, mean travel time, relative increase 171.9%) in some regions. The very few regions with an above-average workload per linac or with limited resilience are recommended to undertake an in-depth analysis of the current workload, workforce, and level of redundancies of the involved ROCs. Potentially, the affected ROCs have already implemented hypofractionation to a larger extent, use orthovoltage devices for benign disorders, or offer specialized linacs for SBRT. All these options free capacities from linacs, enabling treatment of more malignant cases. Consequently, former analyses of linac capacities, such as ESTRO HERO, ESTRO QUARTS, or the MALTHUS project—all of them showing an ideal catchment of about 120,000 residents per linac—need to be adapted to modern techniques and treatment concepts [21,22,23,24, 40].
Notably, this work focused on physical and local events affecting ROCs. Networks for RT planning, whose failure would impact multiple ROCs, were not considered. Furthermore, ROC breakdown was assumed to result in redistribution to the second-closest ROC. This is not necessarily the case, as commercial ROCs might redistribute patients to ROCs of their own network rather than to the second-closest ROC. Also, patient preferences are not included in the model. Lastly, the proposed model does not include changes of traffic infrastructure, namely roads or bridges. These changes could be easily integrated.
Mitigation
As shown in this report, there is excellent spatial accessibility and resilience available in Germany. However, the generation of resilience is based on three cornerstones: the ability to redistribute and absorb the unsatisfied demand, the ability to restore disturbed infrastructure, and implementation of adaptations of in order to increase the resilience to future disruptions [41]. This report focusses on a potential redistribution of patients as a measure of resilience. In most regions of Germany, the second-closest neighboring ROCs can take over patients in case of a local disruption. If this is not possible, three modes of action are recommended:
Patients who are re-referred during their course of treatment currently have limited options for continuing their treatment. Contracts between ROCs, made to ensure resilience, often dictate specific ROCs for redistribution, which may not be the nearest ones. Consequently, patients could experience significant distress and could decide against continuing treatment if travel distances become too long [1, 42, 43]. Technical solutions, such as telemedicine, could ease the transfer of patient data and offer alternatives to the current contract-based resilience system [39].
Secondly, areas with limited redistribution capacities could increase local supply by reducing the mesh size of the local network; hence, by adding new ROCs. This ensures continuous treatment without changing fractionation regimens, indications, or techniques. However, it is costly and requires significant preparation time. Additionally, demographic changes are leading to a reduction in the number of radiation oncologists, thus creating challenges for maintaining the service.
Lastly, an increase in the proportion of hypo- and ultrahypofractionated regimens would reduce the number of patients per day per linac significantly [44]. As a positive side effect, hypofractionated schedules are associated with higher convenience for patients and also reduce the CO2 emissions associated with the total travel distance [36, 45, 46]. Besides these obvious positive effects, an increase in the total number of patients per linac as well as an increase in the complexity of treatments might result in increased wear and tear of the linacs, with a resulting requirement for maintenance and an increase in down-times [47]. Notably, this approach is very cost effective and requires only short times for implementation.
Limitations
Our study is subject to several limitations. First, the assignment to the nearest ROC is based on travel time proximity, which may not accurately reflect the actual travel time due to potential capacity constraints of a given ROC. Hence, patients might be forced to travel to the second- or third-closest ROC. We used a network-based approach focusing on regional capacities to mitigate this limitation.
Second, patient preferences could not be considered. Especially in rural regions, when individual thresholds of travel distances are exceeded, this could lead to decisions against RT [1, 48]. On the other hand, patients in metropolitan regions might choose to be treated at the second- or third-closest ROC, as the time penalty between competing options is low.
Third, our analysis was limited to data from Germany, and cross-border patients may have distorted the picture. Given potential direction-specific reliefs or disincentives, local capacities could be over- or underestimated in these areas. Besides, islands were excluded from the study. However, as only very few inhabitants in Germany live on islands, the influence of this limitation is likely to be limited.
Fourth, we modelled the radiotherapy demand based on health care reimbursement data from 2016, which represent the real incidence of RT in Germany in 2016. Given the easy accessibility to RT due to the high level of insurance coverage as well as the high density of ROCs in Germany, the number of non-treated indications is deemed to be low. Another approach would be to model radiotherapy demand based on cancer incidences, as done for calculating the current and 2050 global and national workforce demand of RT [49]. We decided against the latter approach, as more assumptions would be needed to model RT demand. Furthermore, the granularity of openly available data in Germany is currently too coarse to be included in our analysis.
Fifth, we only considered car traffic, not train/subway or bicycle routes. Especially metropolitan regions have a highly developed commuting system which might modify the catchment area.
Finally, our capacity estimation is based on 40 h/week and frequent use of conventional fractionation. Longer service times per day or week can significantly increase the capacity, and centers in Brazil have documented treatment of more than 900 patients per linac annually [31]. Along these lines, the assumption of three benign cases equaling the workload of one malignant case was chosen in a best guess-manner. A higher ratio would result in higher capacities, while a lower ratio would result in an increased workload. Similarly, a higher proportion of hypofractionation can increase the patients treated per machine. On the other hand, centers with low personnel resources might not be able to further increase their throughput over baseline. Therefore, regions exceeding the assumed maximum number of cases of 800 patients per linac should be reviewed thoroughly in lieu of these limitations. Another factor affecting the estimated capacities is the real disease burden in a given area. Our analysis assumes an equal distribution of disease burden based on the number of inhabitants. However, the age distribution is uneven, with the highest average age in the eastern federal states of Germany. Hence, the workload in areas with an over-average age is at risk of underestimation.

Comments (0)