This study is the first to examine the impact of paravertebral muscle atrophy on recovery from acute work-related low back pain, revealing no significant relationship between paraspinal muscle trophicity, assessed by MRI, and recovery duration. While prior research has predominantly focused on chronic low back pain—demonstrating associations between advanced morphological changes such as muscle atrophy and fatty infiltration with prolonged disability and poorer outcomes [9, 13, 21,22,23] —our results indicate that, in acute cases without underlying structural pathology, muscle condition as evaluated by MRI does not significantly influence recovery time or functional prognosis.
Although a weak association was observed between psoas cross-sectional area and follow-up duration, no significant correlations were identified with other muscular groups. While prior literature has demonstrated a relationship between paraspinal muscle atrophy and chronic spinal conditions, such as degenerative disc disease and spinal instability [9], these associations are predominantly reported in chronic contexts. In contrast, our study specifically excluded individuals with structural abnormalities, focusing on acute, low-energy injuries without underlying pathology. This methodological approach reinforces that, in the absence of chronic degenerative changes, muscular atrophy alone does not appear to significantly influence short-term recovery.
One possible explanation for the lack of a significant association between muscle atrophy and recovery in acute low back pain is that, although structural changes such as muscle atrophy and fatty infiltration can occur in the acute phase [9, 13], their impact on functional recovery may be less pronounced compared to chronic cases. In the acute setting, transient inflammatory responses, nociceptive sensitization, and biomechanical strain may be more influential in determining the duration of disability than morphological changes identifiable on imaging [9, 24].
Our study employed established classification systems—Kader [14], Goutallier [19], and Mercuri [20]—to quantify paraspinal and psoas atrophy. Notably, only higher Goutallier scores in the multifidus showed a modest association with longer recovery, again pointing to the limited influence of structural muscle changes in acute settings. This isolated association may reflect a statistical anomaly, or alternatively, point to differences in the sensitivity and specificity of each grading system. The Goutallier scale may be more responsive to subtle fatty infiltration changes observable in the acute phase, whereas the Mercuri and Kader systems might capture broader or distinct morphological patterns. This discrepancy could also result from inter-scale variability or limited agreement between systems, highlighting the challenge of comparing semi-quantitative assessments in the absence of a validated reference standard for lumbar paravertebral muscles. Overall, these findings suggest that the prognostic value of fatty infiltration grading in acute low back pain remains uncertain and should be interpreted with caution.
The sex distribution in our cohort was skewed, with 77% male participants, who also presented with significantly greater muscle cross-sectional areas. This could reflect sex-based anatomical differences but may also relate to occupational exposure, as men are often overrepresented in physically demanding jobs that predispose to acute LBP. Nonetheless, it contrasts with general epidemiological trends showing a higher overall prevalence of LBP among women [25], suggesting the importance of considering occupational roles in future research.
To our knowledge, no other study has addressed the prognostic role of muscle morphology in acute LBP within occupational health or compensation settings, making these results both original and economically significant, especially given the high burden of acute work-related LBP on healthcare systems and insurance providers worldwide.
Although paravertebral atrophy is frequently identified on imaging, our findings do not support its use as an isolated predictor of functional prognosis or work capacity in the acute post-injury phase. Further research is needed before imaging findings can be integrated into occupational or insurance decision-making frameworks.
This study has some limitations. Its retrospective design is inherently subject to biases, including selection and recall bias. There is also a potential for selection bias related to clinical referral patterns, as patients with recurrent symptoms or pre-existing muscle alterations may have been more likely to undergo imaging and be included in the cohort. In addition, individual variations in occupational demands and leisure-time physical activity were not accounted for, which may have influenced both baseline muscle condition and recovery trajectories. The follow-up period was restricted to the duration of care within workers’ compensation clinics, limiting the assessment of longer-term outcomes.
Regarding image analysis, no inter-rater reliability assessment was performed, which constrains the evaluation of consistency across radiologists. Moreover, only one of the grading systems used was originally developed for paraspinal musculature, and none have been formally validated for use in the psoas or erector spinae muscles. This lack of standardized, validated classification systems specific to lumbar musculature may have limited the precision of morphological assessment and its correlation with clinical outcomes.
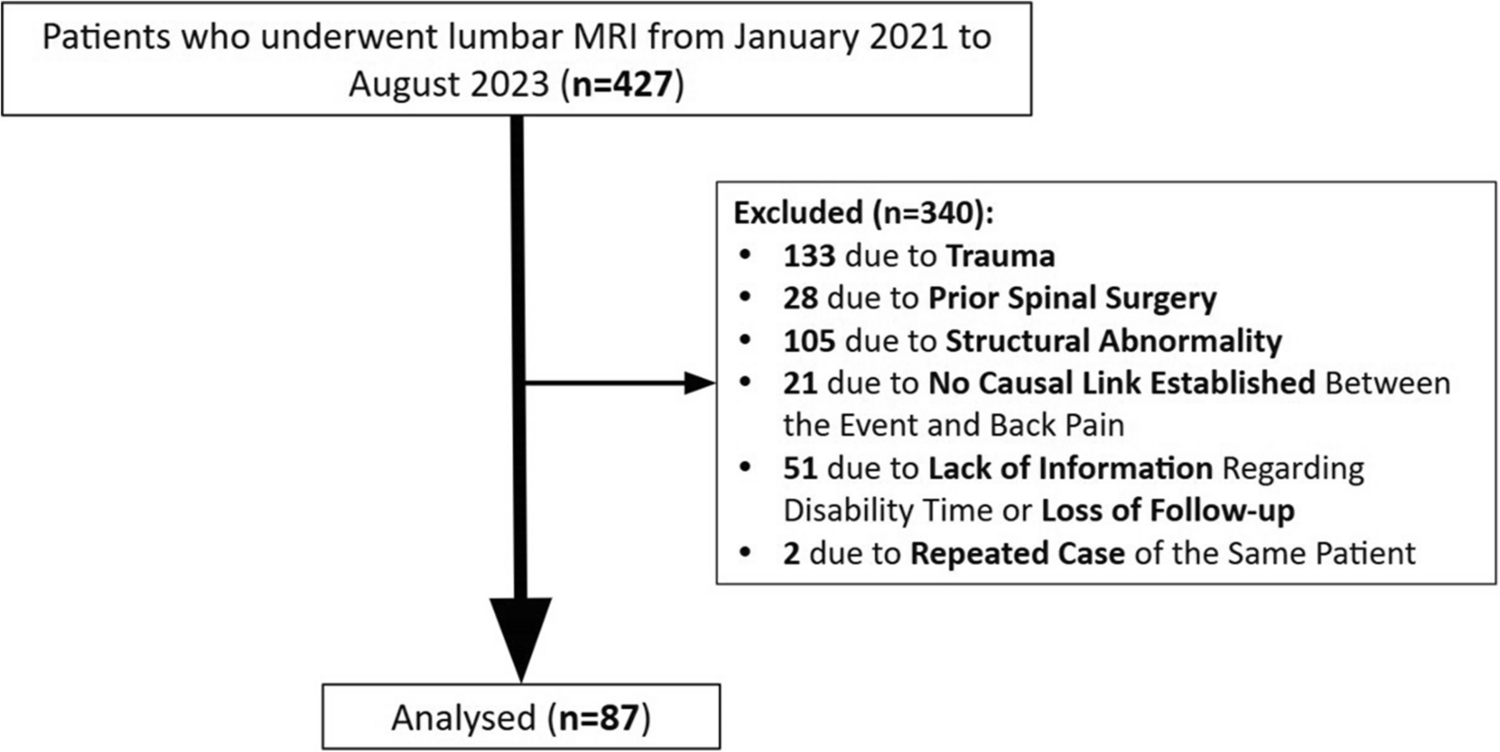
Nevertheless, the use of a rigorous and standardized MRI protocol, interpreted by experienced radiologists blinded to clinical data, combined with a relatively large and well-defined sample of 87 patients, contributes to the reliability and robustness of our findings.
Looking forward, future research should explore the role of paraspinal muscle alterations in the progression from acute to chronic low back pain (LBP) and in the development of structural conditions. The impact of occupational hazards and the risk of recurrence also merit further investigation. To support these efforts, it is essential to develop and validate imaging-based classification systems specifically designed for lumbar musculature, enhancing the clinical relevance of morphologic assessments. Such advances could enable more personalized and effective interventions, ultimately improving patient outcomes and reducing the socioeconomic burden of LBP.
This study found no significant association between paraspinal muscle atrophy and recovery time from acute work-related low back pain. These findings suggest that muscle morphology plays a minor role in acute LBP recovery, contrasting with its known impact in chronic cases.



Comments (0)