
Remember me
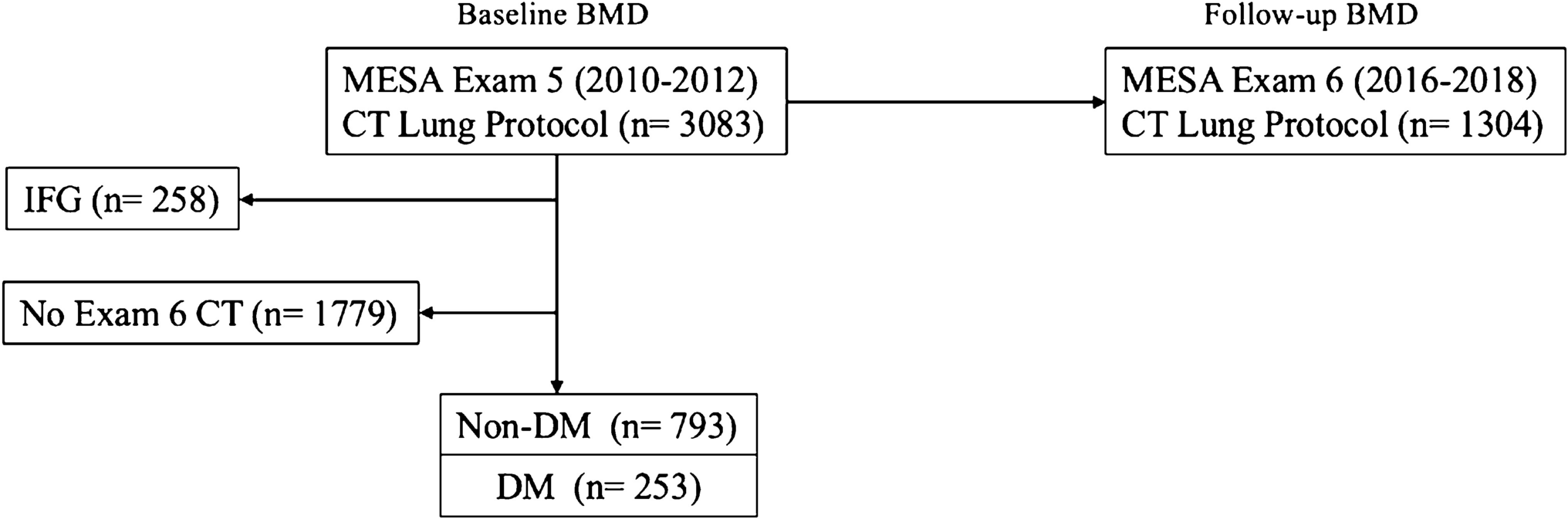
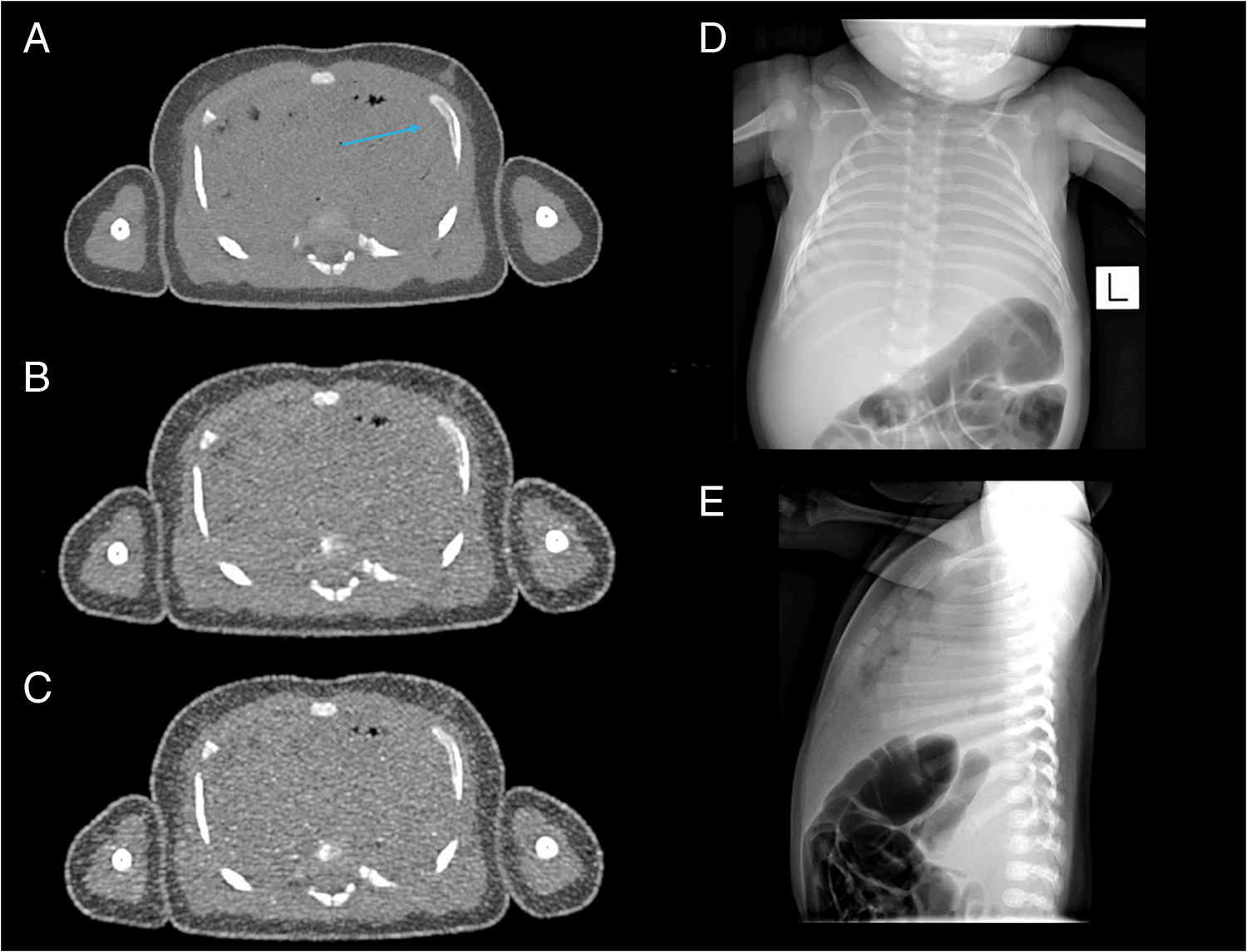
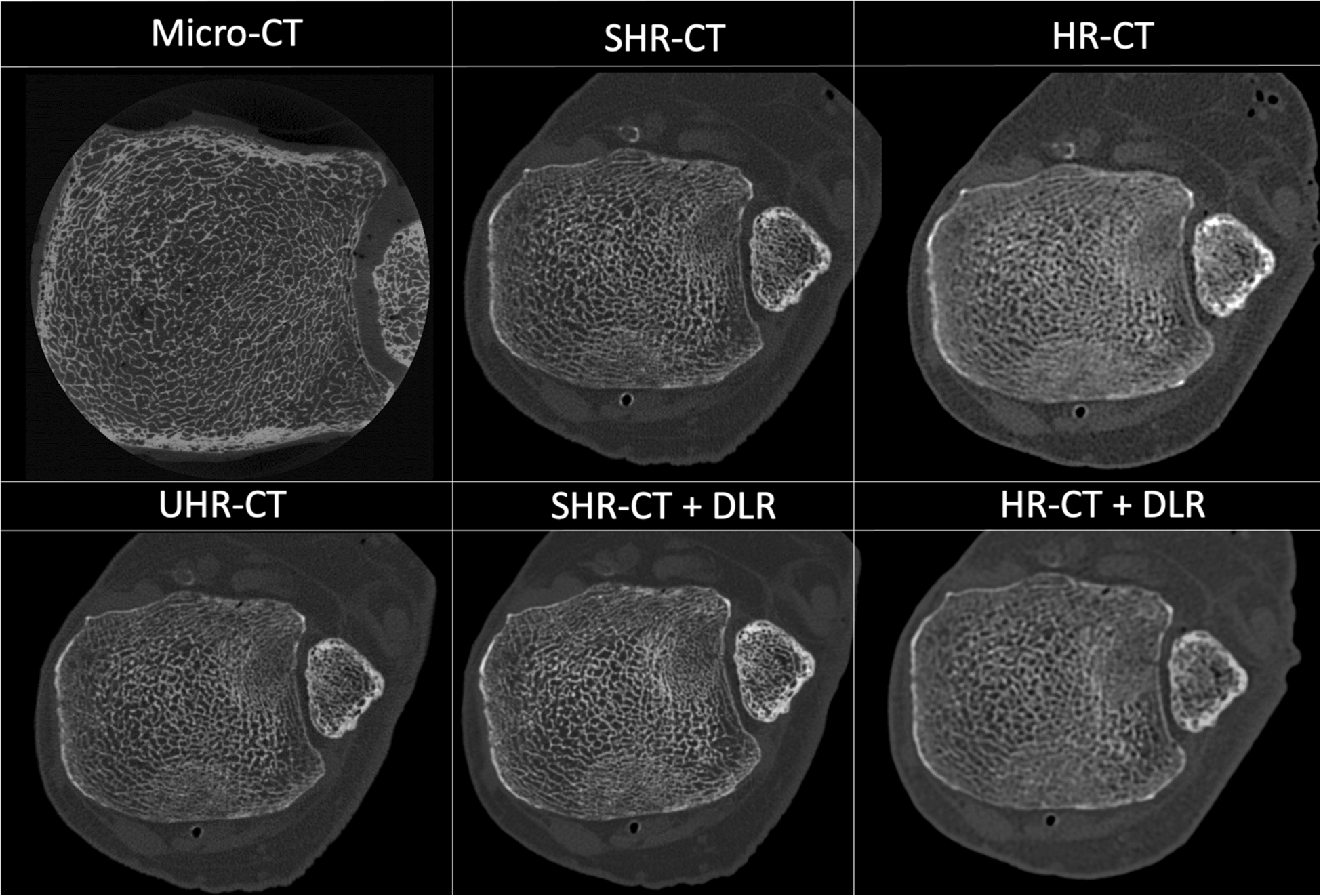
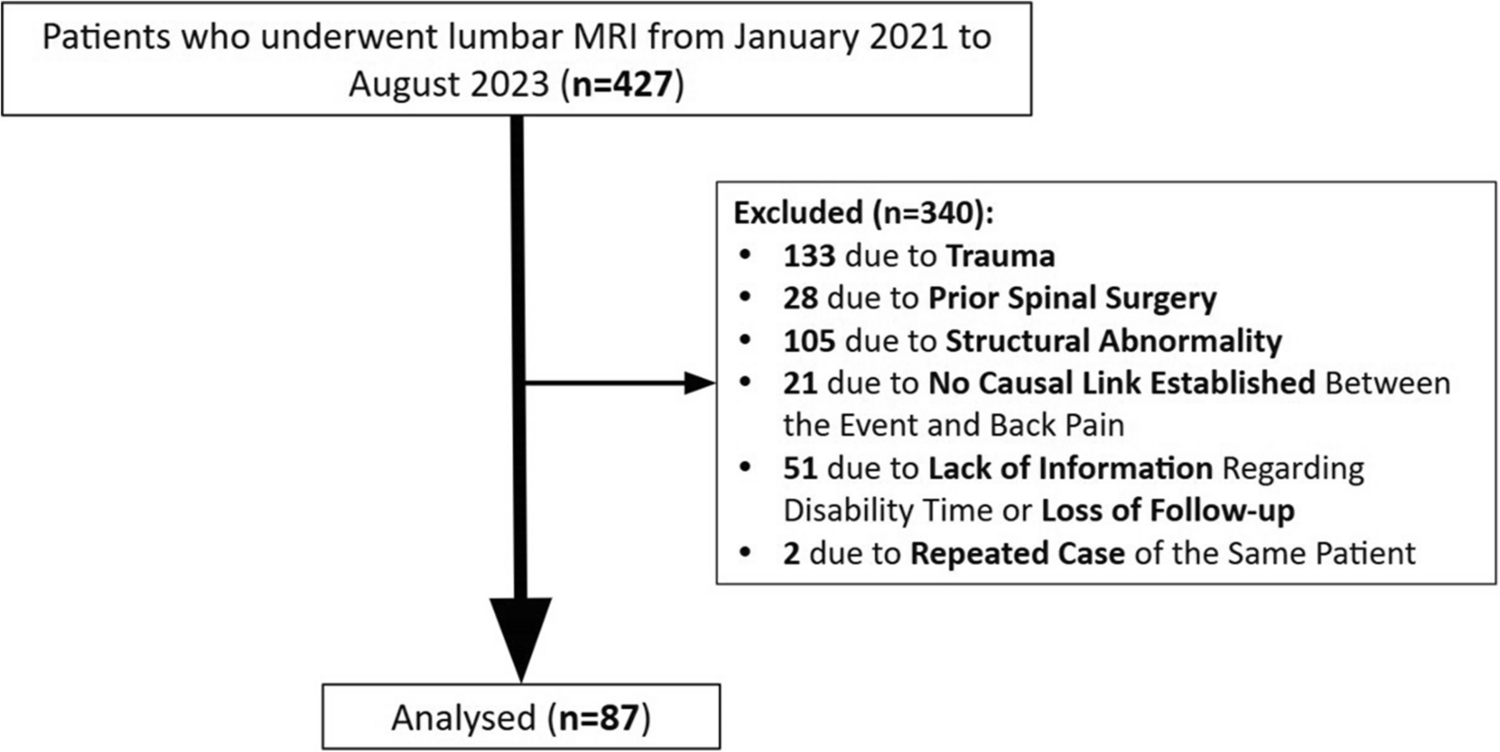

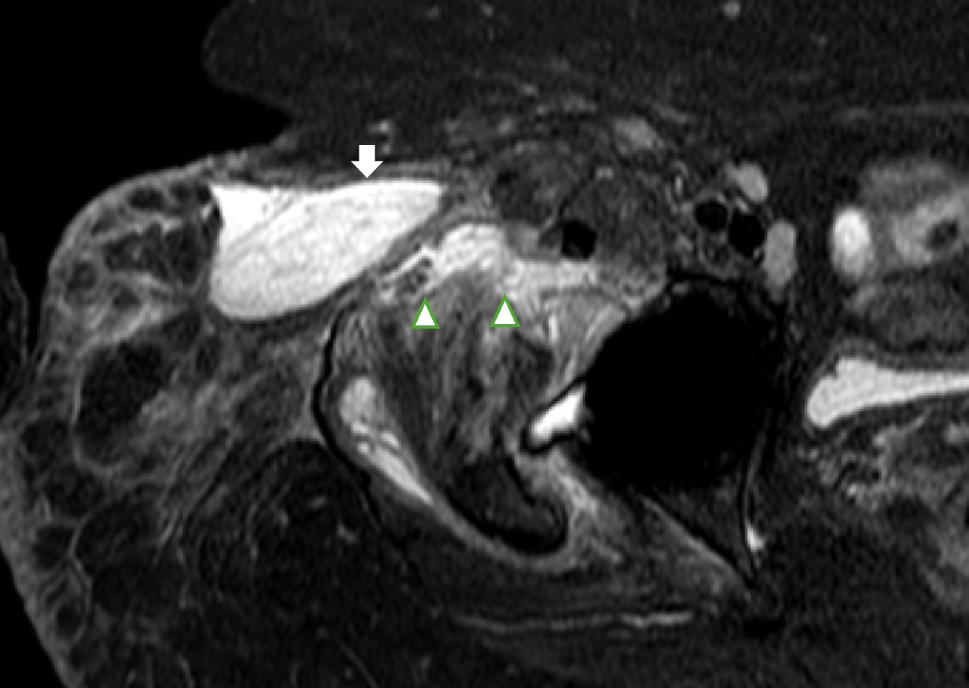

Figure 1 presents the flowchart of the patient selection process. A total of 100 children underwent post-contrast pelvic MRI with reported hip effusion. Hip aspiration was not performed in 57 cases, of which 46 were excluded for the following reasons: positive cultures (n = 15; blood: n = 10, hip effusion: n = 4, muscle abscess: n = 1), prior antibiotic treatment (n = 13), symptoms lasting ≥ 14 days (n = 8), bone marrow edema (n = 2), juvenile idiopathic arthritis (n = 2), incomplete medical records (n = 2), femoral head osteonecrosis (n = 1), trauma (n = 1), Lyme disease (n = 1), and no post-contrast coronal SET1 FS imaging (n = 1). The remaining 11 patients were diagnosed with probable transient synovitis. Hip aspirations were performed in 43 children. Among them, 26 had a WBC count < 50,000 cells/µL. Of these, one had a positive hip joint culture, while 25 had negative cultures. Sixteen of these culture-negative cases were excluded for the following reasons: bone marrow edema (n = 6), prior antibiotic treatment (n = 5), underlying myositis (n = 1), septic knee (n = 1), trauma history (n = 1), granulomatosis with polyangiitis (n = 1), and systemic lupus erythematosus (n = 1). The remaining nine children were diagnosed with transient synovitis. In 17 children with hip aspiration, the WBC count was ≥ 50,000 cells/µL. Of these, four were excluded for juvenile idiopathic arthritis (n = 3) and metallic artifacts limiting the evaluation of femoral head enhancement (n = 1). The remaining 13 children were diagnosed with septic arthritis: three had positive cultures (definite septic arthritis), and 10 had negative hip joint cultures (probable septic arthritis).
Fig. 1
Flowchart of children with septic hip arthritis and transient synovitis; > 50,000 indicates white blood cells per milliliter in the aspirated synovial fluid. eMR, electronic medical records; JIA, juvenile idiopathic arthritis; GPA, granulomatosis with polyangiitis; SLE, systemic lupus erythematosus
Overall, 20 and 14 children were diagnosed with transient synovitis and septic hip arthritis, respectively.
Patient characterizationChildren with transient synovitis had a significantly higher male-to-female ratio (12:8) than those with septic arthritis (3:11; p = 0.038). Additionally, children with transient synovitis were significantly older (mean age: 6.05 ± 2.17 years) than those with septic arthritis (4.2 ± 2.78 years; p = 0.031) (Table 1).
Table 1 Demographic and clinical characteristics of 14 children with septic arthritis and 20 children with transient synovitisFever > 38.5 °C was significantly more prevalent in children with septic arthritis (6/14, 42.9%) than in those with transient synovitis (1/20, 5%; p = 0.012). No significant differences were found in arthritis lateralization, inability to bear weight, or any of the inflammatory indices. However, both the Kocher and modified Kocher scores were significantly higher in children with septic hip arthritis (p = 0.002 and 0.013, respectively). The mean Kocher score was 2.86 ± 0.95 in children with septic arthritis, compared to 1.70 ± 1.30 in those with transient synovitis. The mean modified Kocher score was 2.21 ± 0.80 in children with septic arthritis, compared to 1.20 ± 0.95 in those with transient synovitis. Using the Kocher score, 65% (13/20) of children with transient synovitis had a score of 0 or 1, compared to 14.3% (2/14) of children with septic arthritis. Using the modified Kocher score, 50% (10/20) of children with transient synovitis had a score of 0 or 1 (50%), whereas none of the children with septic arthritis had a score of 0 or 1.
Positive cultures were found in 35.7% (5/14) of patients with septic arthritis (35.7%), originating either from the hip effusion fluid (n = 3), blood (n = 1), or obturator externus abscess (n = 1). All cultures tested positive for Staphylococcus aureus.
MRI findingsTable 2 summarizes the MRI findings. Most patients (78.6–100%) with septic arthritis and transient synovitis exhibited moderate-to-severe (grade 2 or 3) hip effusions. Muscle edema was significantly more common in patients with septic arthritis. Radiologist 1 identified muscle edema in 71.4% of septic arthritis cases, while Radiologist 2 identified it in 92.9% (Figs. 2 and 3) compared to 25.0% and 50.0% in transient synovitis cases, respectively (p = 0.013 and 0.011) (Fig. 4). Additionally, muscle abscesses were identified by one radiologist in two patients with septic arthritis. Both radiologists found only two patients with bone marrow edema, both of whom had septic arthritis.
Table 2 MRI findings in children with septic arthritis and transient synovitisFig. 2
A 6-year-old boy with transient synovitis. The patient developed flu-like symptoms 10 days before admission and presented with 1 day of left hip pain, unable to bear weight on the day of admission. He was afebrile, with a white blood cell (WBC) count of 12,400 cells/mL, an erythrocyte sedimentation rate (ESR) of 43 mm/h, and a C-reactive protein (CRP) level of 3.5 mg/dL. Left hip aspiration yielded a WBC count of 1,150 cells/mL with a negative culture. He was treated with a non-steroidal anti-inflammatory drug (NSAID), resulting in symptom improvement. A coronal MRI STIR shows a large left hip effusion. B coronal MRI SET1 with fat suppression post-contrast shows decreased enhancement of the left femoral head
Fig. 3
A 3-year-old boy with septic hip arthritis and myositis. The patient presented with a 3-day history of fever (38.9 °C) and refusal to bear weight. He had a normal white blood cell (WBC) count, an erythrocyte sedimentation rate (ESR) of 67 mm/h, and a C-reactive protein (CRP) level of 15 mg/dL. Left hip aspiration revealed a WBC count of 11,539 cells/mL, with a positive culture for Staphylococcus aureus. A coronal MRI STIR shows moderate left hip effusion and marked edema in the left gluteal muscles. B coronal MRI SET1 with fat suppression post-contrast shows normal enhancement of the left femoral head and enhancement of the left gluteal muscles
Fig. 4
A 3-year-old girl with septic hip arthritis. The patient initially presented with 3 days of limping followed by a refusal to bear weight. She had a fever of 39.6 °C, a normal white blood cell (WBC) count, an erythrocyte sedimentation rate (ESR) of 80 mm/h, and a C-reactive protein (CRP) level of 4.3 mg/dL. Right hip aspiration revealed a WBC count of 175,000 cells/mL, with a positive culture for Staphylococcus aureus. A coronal MRI STIR shows moderate right hip effusion and edema in the adductor minimus muscle. B coronal MRI SET1 with fat suppression post-contrast shows decreased enhancement of the right femoral head
Only one 53-day-old patient did not have yet a femoral head ossification center. Substantial agreement was found between the two radiologists for the overall determination of decreased femoral head enhancement (kappa = 0.70). Decreased femoral enhancement was commonly observed in patients with septic arthritis and transient synovitis, occurring in 78.6% and 64.3% of septic arthritis cases, and in 45.0% and 50.0% of transient synovitis cases, as assessed by Radiologists 1 and 2, respectively (p = 0.079 and p = 0.495). Based on a consensus read, decreased femoral enhancement was observed in 71.4% of patients with septic arthritis and in 50.0% of those with transient synovitis (p = 0.296). The signal intensity difference between the right and left femoral heads was also not significantly different between patients with septic arthritis (59.1 ± 80.2) and those with transient synovitis (32.8 ± 29.2; p = 0.258).
Sensitivity and specificity of risk factors for septic hip arthritisTable 3 summarizes the sensitivity and specificity of each risk factor included in the Kocher and modified Kocher scores, as well as the MRI findings. As expected, higher Kocher and modified Kocher scores were associated with increased specificity but decreased sensitivity. Decreased femoral head enhancement demonstrated moderate sensitivity (71.4%) but low specificity (50.0%). MRI-detected muscle edema had moderate-to-high sensitivity (71.4% and 92.9%) but moderate-to-low specificity (75.0% and 50.0%) for diagnosing septic hip arthritis, as assessed by Radiologists 1 and 2, respectively. Only one radiologist diagnosed bone marrow edema without muscle edema, increasing sensitivity to 78.6% without affecting specificity.
Table 3 Sensitivity and specificity of risk factors for septic hip arthritis
Comments (0)