
Remember me




This parallel two-arm RCT compared the efficacy of HOP (and TAU) versus TAU alone. The trial was registered before recruitment onset at https://clinicaltrials.gov/study/NCT03218748 and approved by the ethics committee of Ulm University, Germany (Nr. 245/15). Participants were recruited at inpatient, day clinic and outpatient settings of the Department of Psychiatry, Military Center for Mental Health, Berlin, Germany, from 2017 to 2023. Recruitment was delayed by the covid-19 pandemic and because a psychiatric day clinic of the German military, in which recruitment had been planned, unexpectedly closed soon after recruitment onset.
All participants, in both trial arms, received TAU at the Center for Military Mental Health, Berlin, which included psychiatric-psychotherapeutic care tailored to individual needs. Participants received standard outpatient care (weekly guideline-based individual 50-minute psychotherapy sessions and quarterly psychiatric follow-ups) or inpatient/day clinic care (typically two individual psychotherapy sessions per week, sport psychology once or twice a week, movement-based interventions with nursing staff (3×/week), ergotherapy and art therapy (3×/week), and psychoeducation groups on depression, anxiety, and sleep disorders). A proportion of these participants also received trauma-focused interventions (e.g., EMDR, prolonged exposure, or trauma-focused cognitive behavioral therapy). All therapeutic decisions were made independently of study entry or randomization to HOP or to TAU alone. We did not systematically track the exact therapeutic components each participant received, as our focus was on evaluating the added value of the HOP program.
ParticipantsInclusion criteria were current inpatient, day clinic or outpatient treatment at the Center for Military Mental Health, Berlin, Germany, a mental disorder according to ICD-10 and based on chart diagnoses, age 18 or above, sufficient German language skills to participate in HOP, and written informed consent. Exclusion criteria were an intellectual disability (ICD-10: F7); organic disorder (ICD-10: F0); or diagnosis of only a substance- or alcohol-related disorder (ICD-10: F1), without non-substance related current psychiatric comorbidity, since disclosure of substance use disorders is not a topic specifically discussed in this HOP program and the stigma of substance use disorders differs from mental illness stigma [17].
Honest, Open, Proud (HOP): program and group facilitatorsHOP is a peer-led group program that was developed by Patrick W. Corrigan and colleagues in Chicago, US, based on previous work (hopprogram.org [18]). HOP was translated into German in preparation for a previous non-military trial and is called ‘In Würde zu sich stehen’ in German (in English: To stand up for yourself in dignity [19]). HOP supports participants with their decisions whether and how to disclose their condition in different settings; it is not the aim of HOP to make people disclose, but to support an empowered, personal choice, depending on the participants’ goals and their environment. HOP covers the following topics in four two-hour lessons: (i) weighing the pros and cons of (non-)disclosure; (ii) ways of disclosure, from social avoidance and secrecy to selective or indiscriminate disclosure up to broadcasting one’s experience, and finding good people to disclose to; (iii) ways to tell one’s story, if one decides to do so; and (iv) finally, a booster session on participants’ experiences with (non-)disclosure after the third lesson.
Based on our previous qualitative study on disclosure of mental disorders among members of the German military [13] and on participatory research with a group of military servicemembers with lived experience and an advisory panel, we carefully adapted the HOP version for adults to HOP for active military personnel, keeping the overall structure and content outlined above. During this process we replaced the non-military recovery story in lesson 3 of the general adult HOP version by four stories of German military servicemembers, among them one female, and their lived experience of mental illness, covering different disorders and different military ranks. Each HOP group was facilitated by two peers, i.e. military staff with lived experience of mental illness. All group facilitators had been trained by Nicolas Rüsch and had run HOP practice groups with a fidelity of at least 80% prior to recruitment onset. The peer group facilitators received qualitative feedback after the group sessions how participants had perceived the HOP program and whether it was helpful; a summary of this qualitative information is provided in the Results.
FidelityOne research assistant was present in the background of every session and completed the fidelity checklist that was used in previous HOP trials [15]. Fidelity was high with a mean fidelity of 96% for lesson one, 92% for lesson two, 91% for lesson three, and 78% for lesson 4. Mean fidelity across all four sessions was 90%.
Planned sample sizePrior to this study, there was no data on HOP’s efficacy in the military. Based on a power of 80% to detect an effect on at least one endpoint, adjusted alphas of 0.025, and two primary endpoints with an expected correlation of r=−0.3 (unpublished data), 100 participants are sufficient to detect medium effect sizes of d = 0.5 on stigma stress, similar to effects on stigma stress in a previous adult HOP RCT [19], and d = 0.4 on quality of life.
RandomizationAfter completing the baseline assessment (T0), participants were randomly assigned to the intervention (HOP and treatment as usual/TAU) or control group (TAU alone). TAU consisted of inpatient, day clinic or outpatient psychiatric-psychotherapeutic mental health care in the Department of Military Mental Health, Berlin, Germany. The randomization lists and closed envelopes were generated by the Institute of Epidemiology and Medical Biometry, University of Ulm, Germany. The trial was started using a 1:1-randomization; due to the very slow recruitment and the consequent difficulty to fill new HOP groups in time before interested potential participants who waited for the start of a HOP group were discharged, exacerbated by the Covid-19 pandemic, the randomization was changed to a 2(HOP):1(TAU) ratio after recruitment onset. With this 2:1-randomization, it became more feasible to start new HOP groups in time before interested individuals were discharged, and therefore the 2:1-randomization was kept until the trial ended. Blinding of participants was not feasible, and research staff were not blinded as outcomes were assessed by self-report. To reduce the risk of contamination between trial arms, HOP participants were asked not to share HOP materials with control group participants.
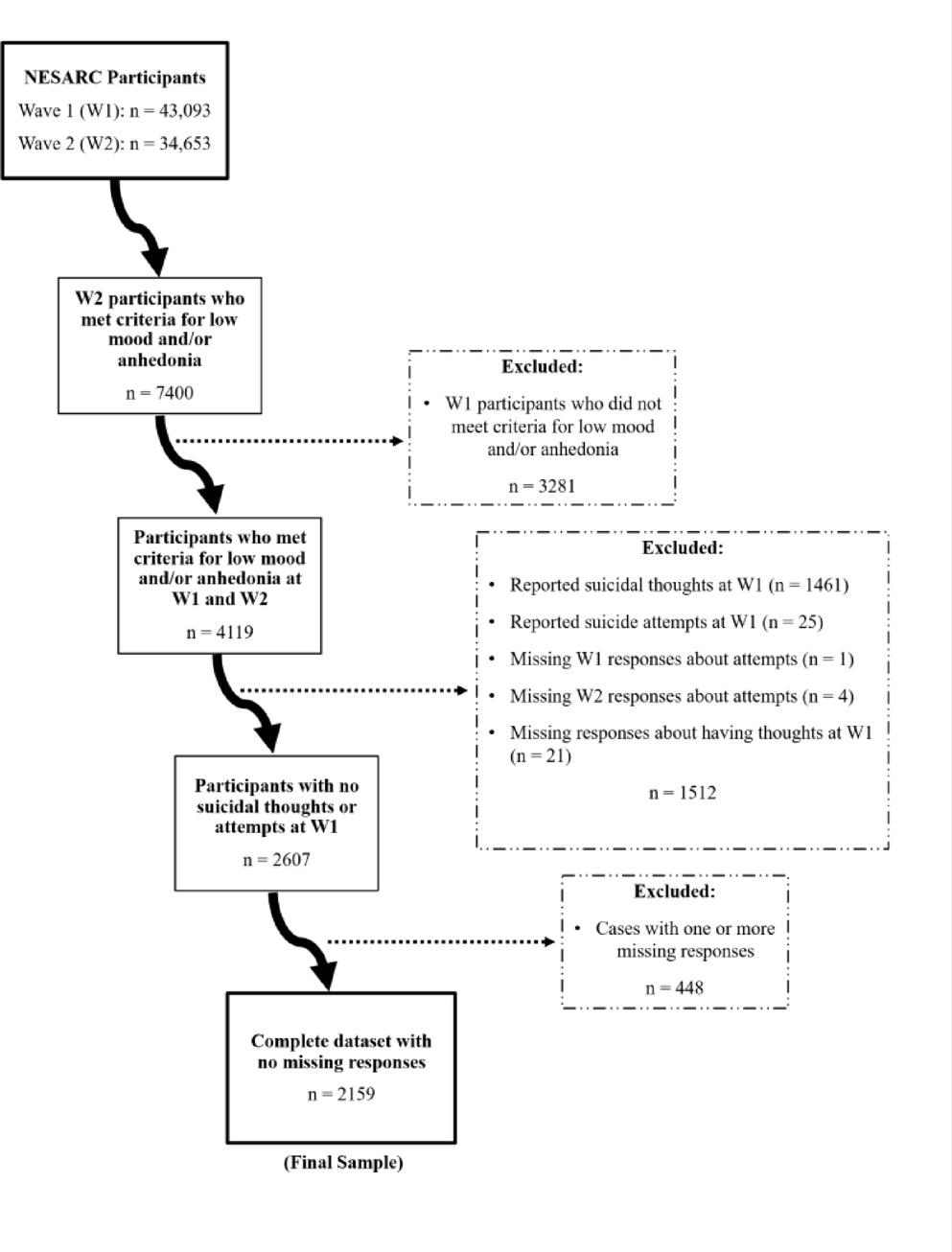
Measures of primary outcomesAll outcomes were assessed four times (see Fig. 1): at baseline (T0), three weeks later (T1, after lesson 3 for HOP participants), six weeks later (T2, after the booster lesson for HOP participants), and finally 12 weeks after baseline (T3). Based on Lazarus’ stress-coping model [20], our first primary outcome, stigma stress, was measured by the 8-item Stigma Stress Scale that consists of two 4-item subscales [21]: the first on perceived stigma-related harm, with higher mean scores from 1 to 7 indicating more perceived harm (Cronbach’s alphas in this study for T0, T1, T2 and T3, respectively: 0.96/0.94/0.95/0.94), and the second subscale on perceived resources to cope with stigma, again with higher mean scores from 1 to 7 indicating more coping resources (alphas 0.80/0.80/0.88/0.88). Stigma stress is calculated as the difference score of harm minus coping resources, with possible scores from − 6 to + 6 and higher scores equaling more stigma stress. The WHOQOL-BREF is a 26-item measure of quality of life developed by the WHO [22], with higher overall raw mean scores from 1 to 5 indicating better quality of life (alphas 0.90/0.91/0.93/0.93). To make scores comparable to the WHOQOL-100, mean scores are multiplied by 4, resulting in mean scores from 4 to 20. The WHOQOL-BREF has four subscales, among them our second primary outcome at T2, psychological quality of life with 6 items (alphas 0.42/0.57/0.45/0.42).
Fig. 1
CONSORT flowchart of trial participants
Measures of secondary outcomesSecondary outcomes were assessed by the 9-item Patient Health Questionnaire (PHQ-9 [23], alphas 0.86/0.87/0.89/0.89), with higher sum scores from 0 to 27 indicating more depressive symptoms; the 18-item Psychological Well-Being Scale [24], with higher mean scores from 1 to 6 equalling higher well-being (alphas 0.68/0.63/0.71/0.67); the 9-item self-esteem subscale of the Rogers Empowerment Scale [25], higher mean scores from 1 to 4 reflecting better self-esteem (alphas 0.89/0.92/0.92/0.92); self-stigma with the 10-item version of the Internalized Stigma of Mental Illness Inventory (ISMI-10 [26] with alphas 0.60/0.63/0.61/0.63 and higher mean scores from 1 to 4 equalling more internalized stigma) and with the Self-Stigma of Mental Illness Scale-Short Form (SSMIS-SF [27]) and its 5-item self-concurrence subscale, higher sum scores from 5 to 45 indicating more self-stigma (alphas 0.76/0.70/0.67/0.75). Four items adapted from previous HOP studies [15, 19] assessed attitudes towards disclosure towards a supervisor at work or towards friends and family as well as towards help-seeking through psychotherapy or psychiatric medication. These items were scored from 1 to 7, higher scores reflecting greater comfort with disclosure or help-seeking, respectively. Secrecy was assessed by the five-item secrecy subscale of Bruce Link’s stigma coping orientation scales [28], with higher mean scores from 1 to 6 indicating a stronger tendency to hide one’s mental illness from others (alphas 0.81/0.83/0.84/0.87).
AnalysesBaseline characteristics of dropouts versus completers at T2, six weeks after baseline, were compared using t-tests or chi-square tests for continuous or binary variables, respectively; the same comparisons were made for baseline variables of HOP versus TAU participants. For the analysis of intervention effects and with two primary endpoints, we corrected the significance level for both endpoints to p < 0.025. All other analyses were exploratory with p < 0.05. Intervention effects were analyzed with analyses of covariance (ANCOVAs) and all available data (complete case analysis), which is more conservative than a per-protocol analysis because participants who had been randomized to HOP but had not participated in all sessions were included (Fig. 1). Intervention effects were tested using group (HOP versus TAU) as categorical independent variable, the respective outcome (e.g., stigma stress at T1) as dependent variable, and the baseline score of the respective outcome (e.g., stigma stress at T0) as covariate. Effect size estimates are provided as partial η², with 0.01, 0.10 or 0.25 indicating small, medium or large effect sizes, respectively [29]. The qualitative feedback of HOP participants was analyzed using a simple content analysis to identify main themes.
Comments (0)