Delay of diagnosis and prolonged duration of untreated psychosis in homeless patients with schizophrenia
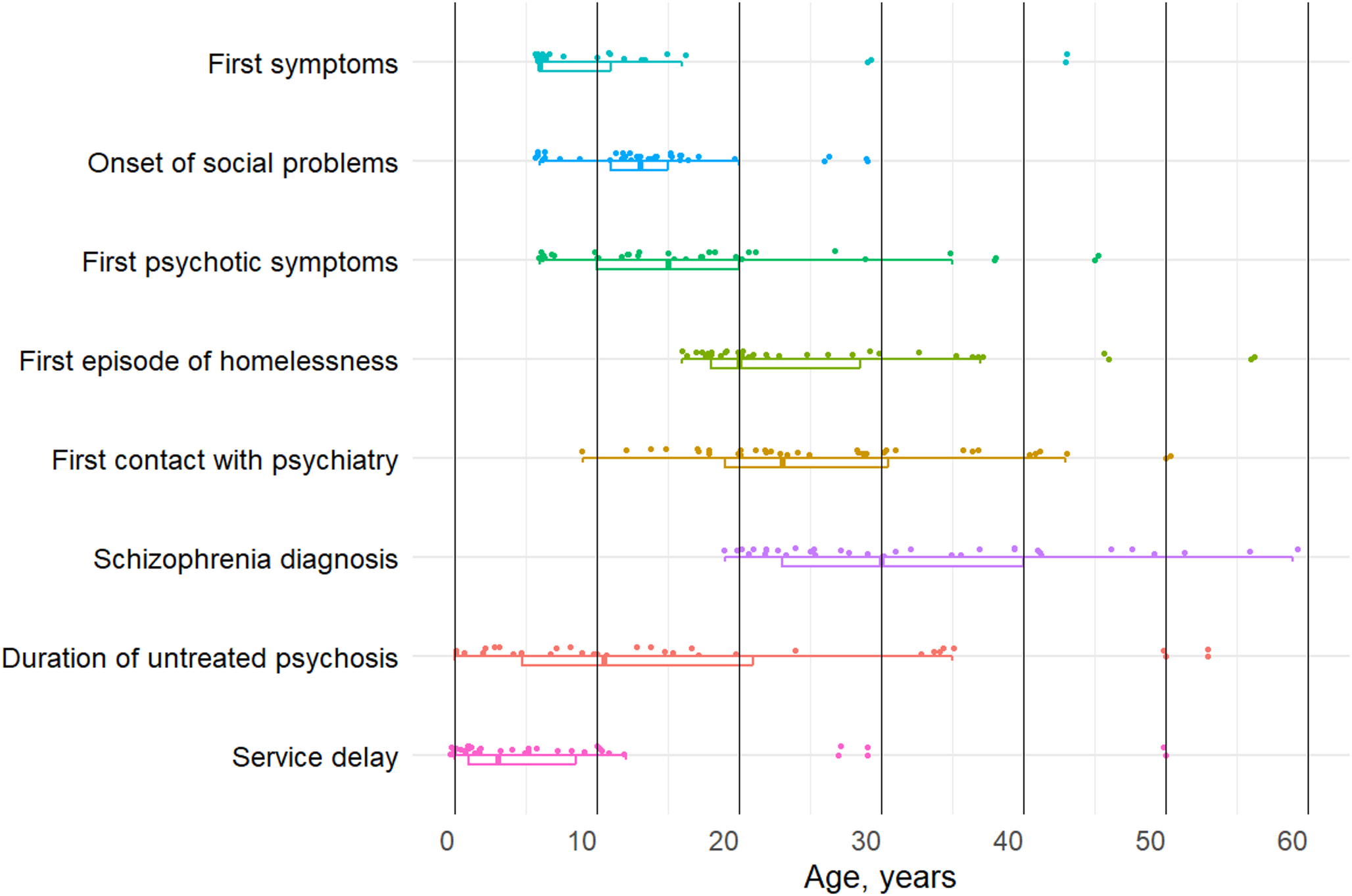
We found an alarming DUP of 15.5 years, with decades spanning from the first symptoms and initial social problems to a diagnosis of schizophrenia, and a delay of 10 years from manifestation of psychotic symptoms to the first contact with psychiatric services.
The delay we identified in this study was markedly longer than previously reported DUP figures — for instance, both a review and a Danish cohort study reported mean DUPs of only 1–2 years in patients with schizophrenia [35, 36], and similarly, a direct comparison with another group of housed patients receiving psychiatric outreach services showed considerably shorter delays [37].
Prior in-depth clinical examinations of homeless patients with schizophrenia
Comprehensive clinical examinations of homeless patients with schizophrenia are rare. To our knowledge, only two prior studies made such comparisons. One is the historical work by Karl Wilmanns [16], who examined 52 mentally ill, homeless individuals—all convicted of at least one crime. Most were diagnosed with dementia praecox (schizophrenia), yet their diagnoses were markedly delayed despite repeated medical evaluations during stays in prisons or workhouses. Their psychopathology was misinterpreted or overlooked for years, with first clear signs of illness appearing at 33.7 years and asylum admission at 41.3 years (based on our recalculation; Wilmanns, 1906b), thus, notably older than our sample [17]. The second study, by Caton et al. and Opler et al. [38, 39], examined 100 sheltered homeless men and 100 never-homeless controls, with a mean age similar to our sample (33.9 years). While Caton did not report on DUP, the homeless group had a reported illness onset at 20 years, which is older than the 13.9 years seen in our cohort, and first hospitalization at 21 years. The homeless group reported more positive symptoms than the controls, but the same level of negative symptoms.
While Wilmann’s study mirrored our pattern of delayed diagnosis, our findings contrast with those of Caton et al., who reported only a one-year gap between illness onset and first hospitalization. Although negative symptoms have traditionally been linked to poor social functioning [40,41,42], neither our study nor Caton’s found them to be more prevalent. Moreover, when we directly compared our present sample to a group of patients with schizophrenia who had stable housing but required outreach services, we found no differences in negative symptoms [43]. This aligns with recent meta-analytic evidence suggesting that all symptom domains contribute similarly to social dysfunction, indicating a broader psychopathological basis than previously assumed [44].
Atypical clinical presentations
While the subtypes of schizophrenia were never intended to define distinct disease entities, but rather to group symptom patterns that commonly co-occur [45], these classifications have largely fallen out of favor in contemporary psychiatry [46]. Yet, as Parnas emphasizes, abandoning these nuanced distinctions has important consequences — particularly for recognizing conditions like disorganized schizophrenia, where the distinctive Gestalt of schizophrenia often escapes the diagnostic radar.
In our sample, we observed a notably high proportion of disorganized, simple, and undifferentiated schizophrenia, with disorganized schizophrenia standing out as especially rare in other populations [47, 48]. Patients with schizophrenia often present with nonspecific or ambiguous symptoms [49], and such unclear clinical pictures can lead to diagnostic delays and prolonged DUP [4]. This challenge extends to institutional settings, where patients diagnosed with schizophrenia during incarceration face longer delays before accurate diagnosis than those diagnosed in the community prior to imprisonment — a pattern the original authors interpret as reflecting these patients’ complex, multifaceted presentations [48].
Consistent with Wilmanns’ early observations [16, 17], a part of the diagnostic delay in our sample may be attributable to these atypical symptom patterns, which required extensive, in-depth assessments to establish an accurate diagnosis—a time- and resource-intensive process that is rarely feasible in routine clinical care [50], especially for marginalized groups like the homeless. This aligns with the notion that a long DUP may not itself directly lead to a poor prognosis but may instead serve as a confounding marker, reflecting the slow and insidious onset of the disorder [51].
Substance use disorder and DUP
Another potential reason for the diagnostic delay could be that the SUD blurs the clinical picture. We found that SUD was present in 54% of our sample, which exceeds the prevalence reported in other samples of individuals with schizophrenia, but is comparable to other homeless populations [10, 52, 53]. However, when examining the DUP and the time from first psychiatric contact to diagnosis, we found no substantial delay in the group with SUD compared to those without; in fact, the SUD group had a shorter DUP, this finding is in keeping with a recent meta-analysis [54], and a study that reported that substance use was associated with fewer psychiatric contacts before appropriate treatment was initiated [55]. It is possible that substance use facilitated earlier contact with professionals who, in turn, helped establish links to psychiatric services.
Relationship between psychiatric disorder and homelessness
In the majority of our sample, symptoms of psychiatric disorder were assessed to be the direct cause of the patients’ initial episode of homelessness. In contrast, only six patients did not show such a direct connection between symptoms of psychiatric disorder and becoming homeless. Yet, in these six cases, symptoms of psychiatric disorder did still contribute to the patient becoming homeless. The presence of psychiatric disorder before the first homelessness episode, potentially playing a key role in this outcome, is supported by studies of homeless patients in Copenhagen in 1992 and Heidelberg in 1906, as well as recent Danish register studies [13, 15, 16]. Early detection and treatment of symptoms of schizophrenia could minimize the risk of these vulnerable patients becoming homeless, however, even in specialized early intervention settings, homelessness is a predictor of poor prognosis [56].
Clinical implications
The diagnostic delays and persistent homelessness described above reflect deep systemic failures in the care of this population. Homeless individuals with schizophrenia, especially those with co-occurring SUD, are frequently overlooked or deprioritized within psychiatric care [18, 57,58,59]. While early detection and prevention receive substantial investment, those who have already fallen through the cracks—arguably the most severely ill—are often left without proper care.
Notably, these patients are not simply disengaged. Consistent with findings from Moulin et al. [60], our results suggest that many actively seek help, often through repeated contact with emergency psychiatric services. Despite an average of seven years in contact with the system—and frequent engagement with child and adolescent services—only seven of our participants had ever received a diagnosis of a primary psychotic disorder, and just two had been diagnosed with schizophrenia. This highlights major missed diagnostic opportunities within routine care.
The consequences are severe. Nearly half of patients with comorbid schizophrenia and SUD had attempted suicide—on average five times each—and many experienced long-term homelessness and lack of recovery [14, 61]. In addition, ten participants had been incarcerated, half for violent crimes, and 13 had exhibited violent behavior from an early age. These findings are consistent with international research showing the heightened risk of imprisonment among individuals with schizophrenia, particularly when homelessness is involved [62]. This cycle of homelessness, missed care, and incarceration underscores the urgent need for more effective detection and treatment strategies for this severely underserved group.
The substantial diagnostic delay and the continuing homelessness in some of these patients despite an accurate diagnosis suggest that the psychiatric system faces major difficulties in taking care of this group of patients. This is reflected in the fact that diagnosing the patients required a team of experienced clinicians, spending several months on interviews, often lasting more than 10 h, and almost half of the appointments missed. The capacity of many current mental health services simply cannot meet these demands, which, however, seems to be needed if we are to care for and properly treat these patients.
The results from our study strongly suggest that mental health staff should be particularly attentive to homeless patients showing up in emergency room or other places within psychiatric services. At least some of the homeless patients do seem to seek help actively: Moulin et al. [60] found that patients with a primary mental health diagnosis and co-occurring SUD or homelessness were more likely to be frequent users of psychiatric emergency departments.
Diagnosing and treating a group of patients with such complex problems require specialist knowledge [18]. Unfortunately, homeless patients with schizophrenia, often with comorbid SUD, seem to be marginalized or stigmatized within mental health services [57,58,59]. While many resources are allocated to early detection and prevention of psychosis, few are spent on treating the persons in the streets, who have fallen through the cracks of society’s support systems, and who indisputably are among the most ill psychiatric patients of our time.
The severe delay in diagnosis and treatment has major consequences for the patients in terms of prolonged suffering, homelessness, and lack of recovery [14, 61].
Future directions
This study exposes major gaps in diagnosing schizophrenia among people experiencing homelessness. Their extraordinarily long DUP—even after years of service contact—points to the need for mobile, outreach-based diagnostic models, especially for those with comorbid substance use. Future work should test how flexible, continuous, cross-sector services that explicitly flag homelessness as a clinical risk factor can shorten delays. Research must also clarify how diagnostic overshadowing [63]—where psychosis is masked by homelessness, substance use, behavioural problems, or insidious onset—derails timely detection, and how training clinicians in core psychopathology plus providing protected time for thorough assessments can counter this. Finally, systematic studies of structural and service barriers to early-stage care for homeless and other marginalized groups are essential.
Limitations
The small sample size is the study’s main limitation and reflects the difficulties in obtaining data.
Although our sample included few women, the sex distribution mirrors that of Danish homeless psychiatric patients, while being slightly younger [10]. Prior research reported higher rates of SUD, non-compliance with anti-psychotic medication, and greater symptom severity in homeless males with schizophrenia; however, differences in symptom severity disappeared after adjusting for SUD and non-compliance [64]. In our study, SUD was linked to a shorter DUP, which suggests that while the male predominance may have resulted in higher SUD rates, a more balanced sex distribution would not necessarily shorten DUP and might even increase it. Nonetheless, the low female representation prevented us from performing sex-based analyses.
While the assessment of the patients involved multiple sources, including electronic health record, prison records, and input from relatives, shelter staff, and nurses, it must be acknowledged that the primary source of information was the patients themselves which entails a risk of recall bias. Not all scales, e.g., SUMD and PSP, have been validated in Danish, but they are widely used in Danish research context [65, 66], and was rated by an experienced clinician.
Due to the extensive test battery, the psychopathological rating scales were not administered on the first day, and scales such as the EASE were sometimes completed over multiple sessions.
Conclusion
Our findings indicate that modern healthcare and support systems are poorly equipped to diagnose and care for this highly vulnerable group of patients with schizophrenia. There is a pressing need for greater attention to homeless individuals with schizophrenia—before, during, and after their contact with psychiatric services. Particular vigilance is required when homelessness is combined with key risk factors such as prior violence or criminal behavior and comorbid SUD. Finally, ensuring that clinicians have the specialized skills to recognize and diagnose the complex, often atypical clinical presentations seen in this group is essential for improving outcomes and reducing long-term harm.

Comments (0)