In this study, we used intersectional MAIHDA models to assess whether a schizophrenia diagnosis, along with compounding and interacting axes of social marginalization, was associated with lower HIV testing and reduced engagement in the HIV continuum of care. Prior to adding fixed effects to the model, nearly 13% of the variability in HIV testing could be attributed to intersectional strata based on schizophrenia diagnosis, race/ethnicity, sex, and age. Even after adding fixed effects to the model, 1.4% of the variability in HIV testing could still be attributed to intersectional position, highlighting the persistent influence of social positioning on HIV testing behavior. Further analysis detected intersectional effects for 19 intersectional positions; that is, the predicted mean prevalence was greater or less than the expected mean prevalence based on additive combination of covariates. In contrast, our analysis of inequities in retention in care found little evidence for intersectional effects, as less than 1% of the variability in retention could be attributed to intersectional positions.
Contrary to our hypothesis, we did not find that a schizophrenia diagnosis, or most intersectional positions that included a schizophrenia diagnosis, was associated with lower HIV testing and retention in care. In fact, MAIHDA models with fixed effects revealed that a schizophrenia diagnosis was associated with a greater likelihood of both having an HIV test within the past year and being retained in HIV care, a finding that has been reported in some earlier studies [34, 39, 40]. A closer examination of intersectional positions, however, point to potential gaps in care for older Black men with schizophrenia, who were retained in care less than expected.
The results indicating lower than expected retention in HIV care among older Black men with schizophrenia warrants further investigation. Little exists in the literature on the unique challenges experienced by this specific intersectional position. However, previous studies have identified low rates of engagement in HIV care among Black men who have sex with men (BMSM) as well as low rates of engagement in psychiatric care among Black men with schizophrenia [41, 42]. In a qualitative study evaluating the experience of BMSM clients with integrated behavioral and clinical health care services at eight demonstration sites across the United States, Daniels et al. identified various barriers to optimal engagement in HIV care among BMSM [42]. Perceived stigma and discrimination emerged as a prevalent theme for care disengagement, with clients noting that they were being perceived “differently” due to their identities (racial identity, sexual orientation, and HIV status). This was connected to experiences of judgement, inadequate provider sensitivity, and breaches of confidentiality, all of which damaged the patient-provider relationship. These experiences of intersectional stigma could be compounded with a schizophrenia diagnosis and make managing them more challenging. Wagstaff et al. note high rates of HIV care disengagement and disengagement from adult psychiatric outpatient services across multiple countries [43]. In their qualitative study of Black male patients with schizophrenia in the UK with a history of disengagement from mental health services, the authors note the stigma of being associated with mental health services as having a detrimental effect on their relationship with their community. Participants also felt that mental health services were “coercive,” “hounding” them about their medication. In addition to intersectional stigma, compounding structural barriers such as lack of transportation and inflexible or inconvenient work schedules likely also impact lower engagement in HIV care for older Black men with schizophrenia. Daniels et al. also noted that BMSM clients highlighted telehealth appointments as a convenient option to overcome such barriers and as less alienating with respect to the intersectional stigma they experienced during in-person medical visits. The recent expansion of telehealth visits in response to the COVID-19 pandemic should be studied for its potential impact on narrowing the retention in HIV care gap for this intersectional position. Separately, the growing body of evidence showing that Black men are misdiagnosed with schizophrenia at higher rates compared to other groups might also contribute to our findings [44,45,46]. The high rates of false diagnoses of schizophrenia among Black men signals racial discrimination in the healthcare system and can result in medical mistrust among patients. While we cannot, with this study, empirically speak to the attributable risk of medical mistrust on HIV care disengagement for older Black men with schizophrenia, further investigation is warranted.
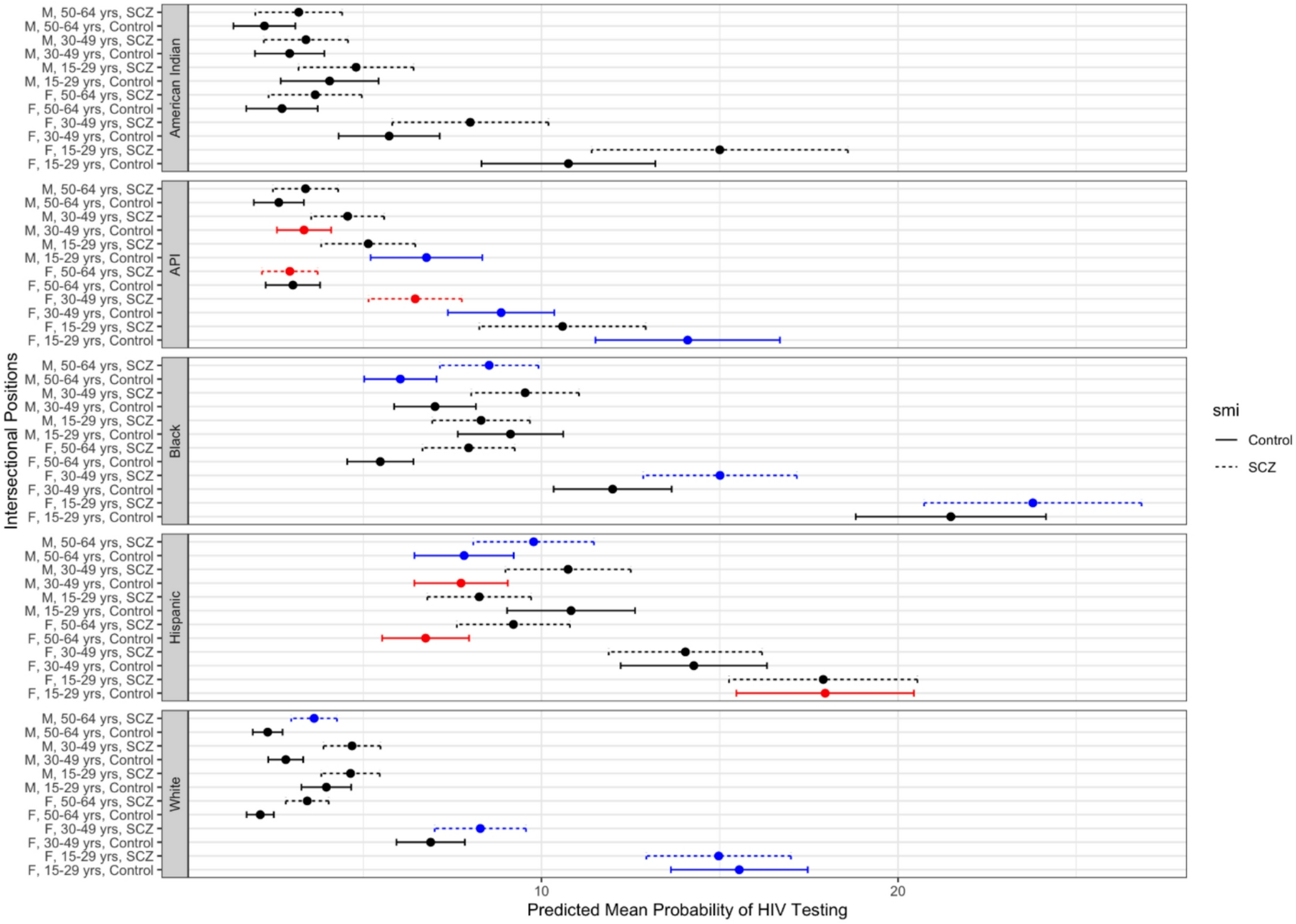
Mapping the distribution of risk between groups and outcomes facilitated interesting contrasts that might otherwise go unnoticed using a “single axis” approach. For example, young (ages 15–29 years) Black females with schizophrenia had the highest predicted mean prevalence of HIV testing among all the intersectional positions. Their predicted mean prevalence also showed evidence for synergistic intersectional effects (i.e., the predicted mean prevalence was greater than expected based on additivity). In contrast, White males without schizophrenia (across all age groups) had among the lowest predicted mean prevalence of HIV testing. These differences may speak to differences in risk perception by individuals and their care providers. However, when exploring inequities in retention in care, we found that older White males without schizophrenia, a group that likely experiences the least marginalization and structural oppression, were among the most likely to be retained in care and had a higher-than-expected predicted mean prevalence. Younger Black females without schizophrenia, on the other hand, were among the least retained in care and had a lower-than-expected predicted mean prevalence. This could signal reduced access to health care services or other barriers to care that must be removed.
Our multivariable regression modeling (Model 2) reveals several notable trends: Medicaid beneficiaries with SMI (compared to the control group) were more likely to have an HIV test and to be retained in HIV care; females (compared to males) were more likely to test for HIV, but less likely to be retained in HIV care; and there was a dose-response relationship with respect to age, where older individuals were less likely to get an HIV test but more likely to be retained in HIV care. Black and Hispanic individuals were more likely (compared to White individuals) to test for HIV, but no differences were observed for retention in HIV care. These trends are consistent with the past 12-month HIV testing results from the 2012 Behavioral Risk Factor Surveillance System survey [47]. The intersectional lens provided by MAIHDA models lends further nuance to this examination of heterogeneity of vulnerability. For example, while younger people were more likely to have an HIV test, this trend was most pronounced among females. Across racial and ethnic groups, the predicted prevalence of HIV testing was largely similar for males regardless of age.
The intersectional MAIHDA approach is a useful tool for identifying priority populations and addressing HIV and related disparities in the US. Our results also highlight the low testing among both American Indians and API groups (across intersectional positions)-- groups often relegated to the racial category of “Other.” Our models specifically call attention to the low prevalence of testing among men in these groups as well as older women. Among API, specifically, middle-aged men and older women with schizophrenia not only had among the lowest HIV testing prevalence, but testing among these groups was also lower than expected. Further investigation is warranted to understand if this low prevalence of HIV testing is due to structural barriers or low risk perception.
Our findings should be understood in the context of several important limitations. First, our analysis is based on Medicaid claims data. Billing data are used as a proxy for what occurred during the medical visit but does not reveal what is in the actual medical record. Especially with respect to retention in HIV care, we are limited in not having viral load data, which is the most accurate assessment of a person’s HIV care. Services that are not billed, such as HIV testing in community settings, are not captured in this dataset. Second, our use of the CDC’s definition of retention in care, and restricting our analysis to the 2012 calendar year, risks under-counting the number of people retained in care if they received at least two care visits at least three months apart within twelve consecutive months, but those months straddled two calendar years (e.g., 2011 and 2012, or 2012 and 2013). Third, claims data do not include measures of sexual orientation, gender identity, or substance use, which are all highly relevant in the epidemiology of HIV and be additional cofounders impacting access/engagement. Fourth, due to delays in Medicaid data availability, we were constrained to use data from 2012 as the most recent available data. However, given that our study is framed around intersecting structural inequities, the testing and care dynamics observed likely persist well after this data was collected. Recent developments in MAIHDA models propose expanding its functionality to include random slopes which, in our case, could allow for the investigation of differences in trends over time by intersectional position (i.e., difference in differences) [48]. Given wide variation in state-level HIV testing among this population across states [34], another proposed development is the inclusion of random coefficients, which, in our case, could be applied to assess differences in intersectional positions by geography. The latter may be useful in further understanding the impact of context and structural disadvantage when studying disparities in the HIV care continuum, especially with respect to states that did not expand Medicaid coverage. For example, non-expansion states may only cover “medically necessary” HIV testing, wheras states with expanded Medicaid coverage will also include “routine” HIV screening (i.e. HIV testing offered to everyone between the ages of 13 and 64, regardless off perceived risk) [49]. Lastly, the use of Medicaid claims data means that our results cannot be generalized to the broader US population, including uninsured or commercially insured individuals. Relatedly, services not billed to Medicaid, such as HIV testing in community settings, is not captured in our data. Our inability to examine these services could result in an underestimation of HIV testing for some intersectional positions, particularly those more likely to be uninsured. However, our results are relevant to the broad population of people with SMI because an estimated 67% of people with diagnosed schizophrenia access medical care through Medicaid and speaks to a population with greater unmet needs given the relationship between Medicaid coverage, income, and disability [50].
The intersectional MAIHDA approach is a useful tool for identifying priority populations for federal efforts to address the HIV epidemic and the hardest hit communities [51]. HIV testing and care interventions often take a “single axis” approach; that is, targeting outreach efforts towards single identities (racial, sexuality, gender identity, mental health status). While our models show that these variables were independently associated with HIV care outcomes (when included in the model as fixed effects), the results also indicate that there was remaining variability explained by the random effects and, therefore, an intersectional (“matrix”) approach may also be warranted. Specifically, our intersectional MAIHDA models identified older Black men with schizophrenia as an especially vulnerable group with lower-than-expected retention in HIV care. This could be the result of compounding structural barriers to care as well as perceptions of intersectional stigma. This should be investigated further, along with testing interventions such as telehealth, to close the gap in the HIV care continuum.

Comments (0)