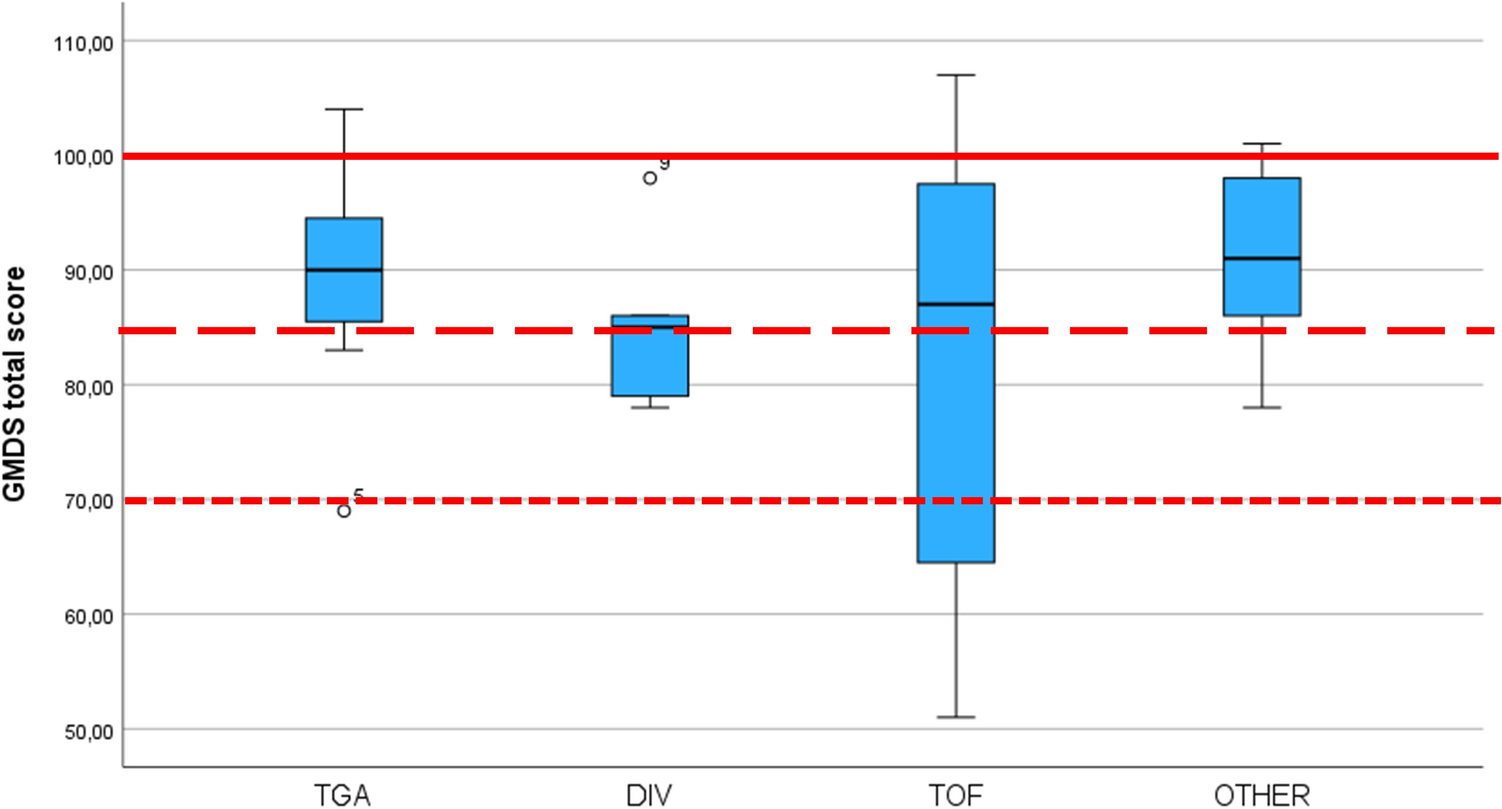
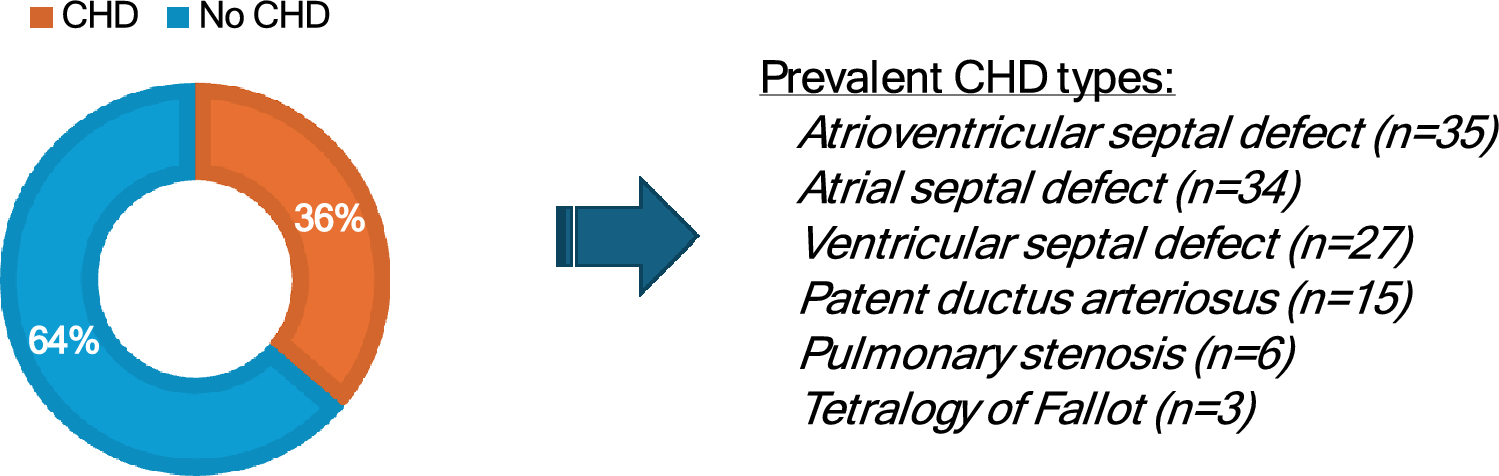
In this study, we compared the EEG spectral power of infants with congenital heart disease (CHD) after cardiac surgery to that of healthy controls. We found significant differences between the two groups in the percentages of alpha and beta frequencies. Furthermore, the EEG spectra of the CHD group did not show the typical age-related changes that characterize normal neurodevelopment. Psychomotor development assessments revealed that 7 out of 35 CHD children (20%) had borderline GMDS total scores, while 3 out of 35 (5%) had impaired results. However, GMDS scores did not correlate with the EEG.
The increased power in the medium-to-high frequency ranges in the CHD group was sustained and particularly pronounced in some children compared to controls. The origin of this abnormal increase is unclear. A similar pattern of diffuse frequencies, ranging from high alpha to low beta, is typically seen with certain sedative medications, particularly benzodiazepines and barbiturates [24]. However, in the CHD group, all children had discontinued sedatives at least five days prior to EEG recording, making a drug effect or rebound unlikely.
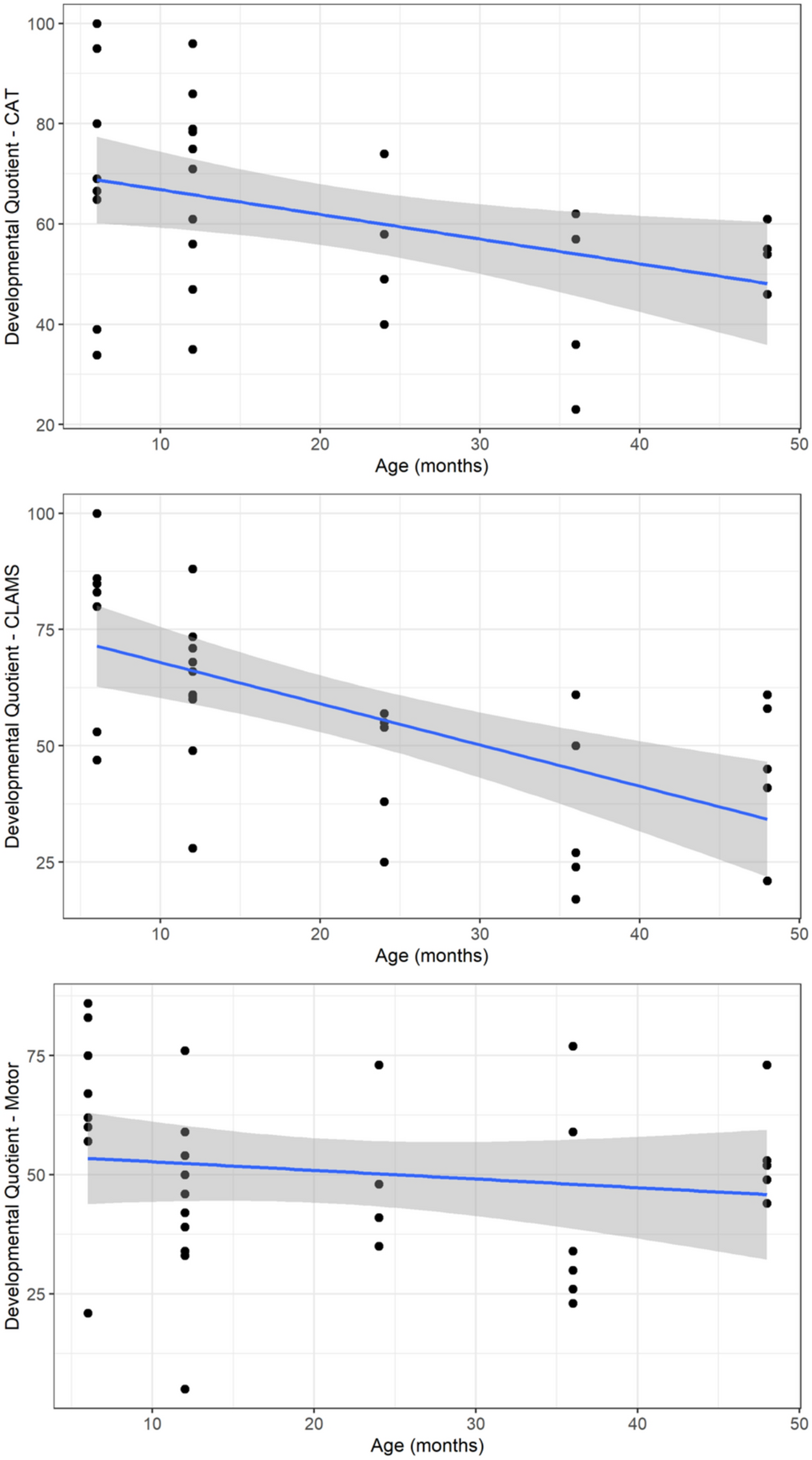
This increase in medium–high frequencies is probably generated by abnormal cerebral oscillations. This may also explain the absence of typical maturational changes in the ratio between frequency bands, which are usually evident during the first year of life. In normal development, the predominant low frequencies characteristic of the neonatal period are gradually replaced by emerging higher frequencies [25, 26]. This trend was evident in the control group, where increases in theta, alpha, and beta bands were significantly associated with age.
Several previous studies have investigated the role of EEG in detecting brain injury or delayed maturation (for a review, see [27]). However, these studies often rely on qualitative visual EEG analysis or amplitude-integrated EEG, which provide different information compared to our spectral power-based methodology. Studies using spectral power to estimate coherence or connectivity have found increased high-frequency connectivity. Markus et al. (2021) observed a distinct emergence of alpha and beta activity, interpreted as an increased inhibitory neuronal function [28]. In another study, a similar increase in high-frequency EEG connectivity was associated with brain injury and immaturity [18]. High-frequency oscillations are thought to support local processing, segregation, and differentiation within specialized cortical regions, while low frequencies support global, distributed processing and integration between distant cortical areas [29].
Therefore, increased high-frequency connectivity in CHD neonates may suggest stronger cortical differentiation but reduced integration across distant brain areas [18]. We didn’t measure connectivity, but in our patients, the high proportion of high alpha/low beta activity could represent a neurophysiological signature of an imbalance in the “local vs. distributed” organization of spontaneous brain networks, possibly reflecting compensatory mechanisms. This shift in frequency content may also indicate a reduced response of local neural populations to global modulatory influences, which are crucial for large-scale integration [25].
The origin of this high-frequency increase remains unclear, in part because a major limitation of our study is the lack of pre-surgery EEG recordings. Previous literature comparing pre- and post-surgical EEGs, mainly based on visual inspection, found a variable percentage of abnormalities before surgery and a marked increase afterward [30,31,32], suggesting a significant role of surgery and related procedures in generating EEG abnormalities.
The incidence of EEG abnormalities varies across studies [30, 31, 33,34,35], likely reflecting the complex and heterogeneous etiologies underlying brain dysfunction. CHD infants are at risk of hypoxia, neuroinflammation, stress, and procedures involving general anesthesia. There is evidence that CHD and its associated factors can lead to early structural and microstructural brain abnormalities, with immediate functional consequences observable as altered neuronal network connectivity (Birca). The elusive yet crucial ability of EEG to detect such abnormalities is supported by its predictive power for later cognitive outcomes (see [36] for a review).
Efficient fine-tuning between local and distributed networks is crucial for cognitive development and it is reflected in the balance of high- and low-frequency EEG components. Alterations in this balance may predispose the CHD brain to later neurocognitive and neuropsychological impairments. Early disruption of neuronal network development, if sustained, could underlie the persistent cognitive deficits observed in CHD survivors [37]. Even in the absence of overt brain damage, subtle functional abnormalities in developing circuits may interfere with cognitive milestone acquisition. Moreover, this could impact the maturation of later-developing networks, particularly fronto-subcortical circuits critical for higher cognitive and psychological functions [38].
Thus, in the absence of targeted interventions, disrupted brain circuits may accumulate during development, leading to a cascade of adverse effects on later cognitive functioning. Once consolidated, an altered pattern of functioning may become a stable trait, as shown by long-term follow-up studies in adolescence and adulthood [39, 40]. In children with CHD, cognitive difficulties have been reported throughout infancy, childhood, and adolescence [5]. Early language acquisition and behavioral self-regulation issues [30, 41, 42] may evolve into academic, cognitive, and socio-emotional challenges in school-age children. Specific difficulties in attention, executive functioning, visuospatial processing, processing speed, and social cognition have been documented [2, 4, 6, 43]. Children with CHD are also at higher risk for psychiatric and neurodevelopmental disorders, including mood and anxiety disorders, ADHD, autism spectrum disorder, and learning disabilities [44,45,46,47]. Furthermore, even patients with average intelligence and no motor impairments may present subtle neuropsychological difficulties or psychological disorders [48, 49]. These impairments can negatively impact academic performance and social life, leading to long-term effects on adult socioeconomic status and career outcomes [9].
However, brain maturation, including network refinement and myelination, continues throughout childhood, providing a significant opportunity for recovery. This underscores the importance of a lifespan approach to improving outcomes in CHD patients and the importance of supporting the achievement of early developmental milestones that underlie the maturation of more complex cognitive abilities.
Evaluating the emergence and characteristics of spectral EEG components—and their deviations from the expected developmental trajectory—may be crucial for understanding early brain development abnormalities. In a previous study on children with a history of prematurity, we found an association between neonatal spectral EEG data and neurocognitive performance at six years of age, suggesting that spectral features may serve as a useful risk biomarker [50]. As a confirmation of the usefulness of neurophysiological techniques, we found a predictive ability also in other clinical settings and with other methodologies similar to the EEG [51–53]. In the present study, results seem to support the potential role of spectral EEG, although only long-term follow-up will clarify the clinical significance of the identified differences. Once at-risk children are identified, they could be placed in a more stringent and longer neurological and neuropsychological monitoring program. Viewed from a clinical practice perspective, performing an EEG is inexpensive and non-invasive. Using spectra analysis would also mean that specialist personnel would not be required, as it would be easily quantified. Detailed clinical evaluations with a focus on neuropsychological and psychological domains offer promising avenues for future neurological and neurobiological research, even in the challenging population of CHD infants without overt brain injury, in which prognosis is particularly difficult.
In the present study, most children (71%) demonstrated normal psychomotor development. However, the young age of the participants may have limited the sensitivity of the GMDS in detecting subtle atypical developmental trajectories, as noted in other clinical contexts [51]. This may also explain the lack of association between EEG findings and GMDS scores. Nonetheless, GMDS scores were associated with certain clinical factors; in particular, poor GMDS outcome was associated with longer surgery durations and shorter rewarming times during cardiopulmonary bypass (CPB). Longer surgery time may reflect more severe medical conditions or may itself contribute to developmental delays due to the cumulative impact of procedures and associated stressors on the brain.
This study several other limitations. The control group was recruited retrospectively rather than prospectively, requiring the use of normative samples for GMDS interpretation. Despite experiencing hospitalization for non-CHD conditions, the control group may still differ in key aspects such as hospitalization stress, unfamiliar environments, or anxiety. The same EEG methodology was, however, used for both groups. Additionally, our CHD cohort was clinically heterogeneous and too small to examine the effects of multiple clinical variables. Important insights into CHD-related brain development could be provided in future research by comparing CHD patients with other clinical populations (e.g., preterm infants). Thus, regarding the evaluations, only a single EEG and GMDS assessment was conducted, and the study lacked longitudinal follow-up.
Finally, MRI was not performed in all patients, raising the possibility that certain abnormalities—such as subtle signs of cerebral immaturity or microhemorrhages, which may be less evident on cranial ultrasound but potentially relevant to EEG spectral changes—were not documented. Future studies would benefit from investigating the relationship between EEG abnormalities and MRI findings.

Comments (0)