The Predictive Role of Prenatal Echocardiography in the Diagnosis of Postnatal Pulmonary Stenosis
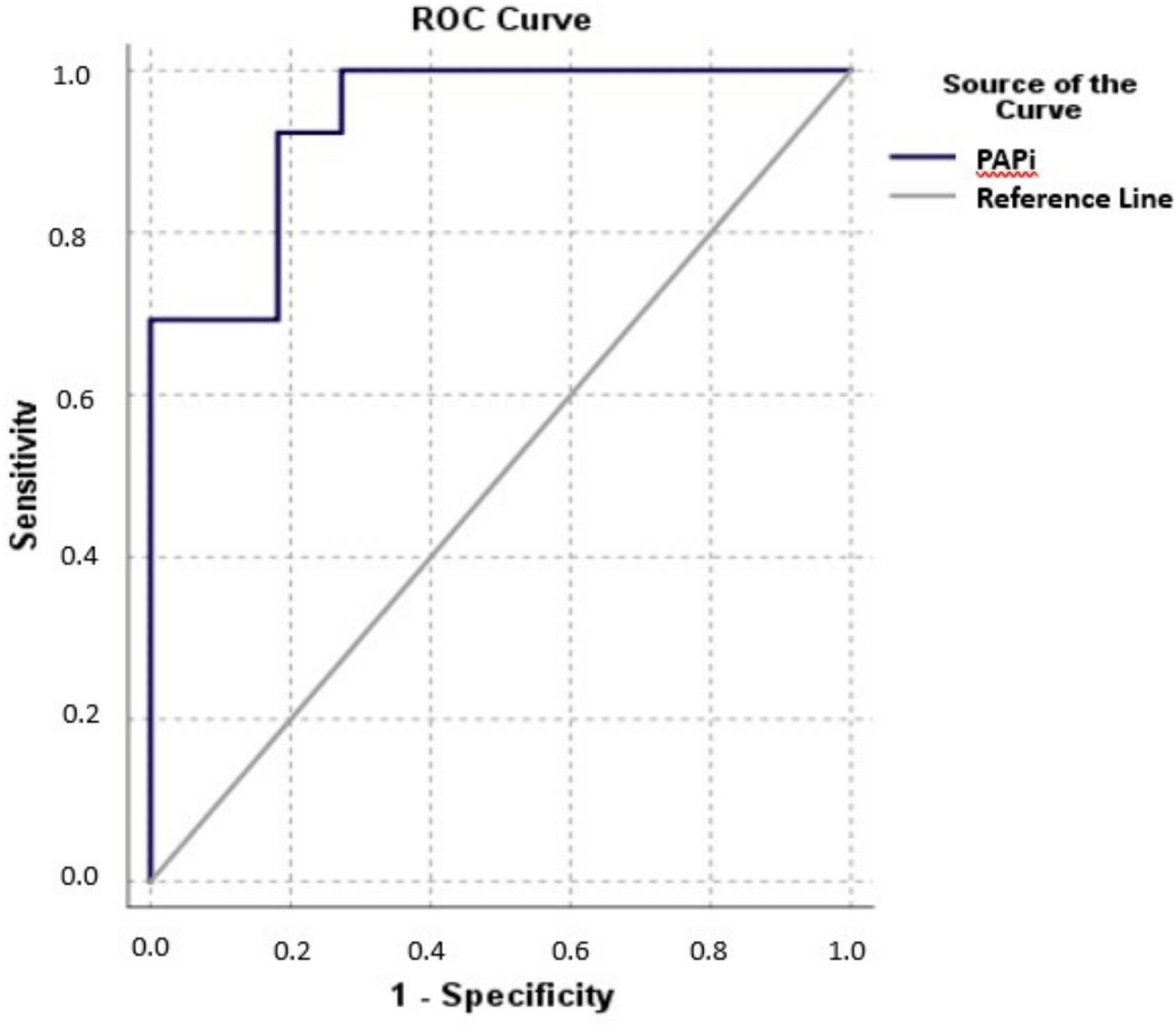
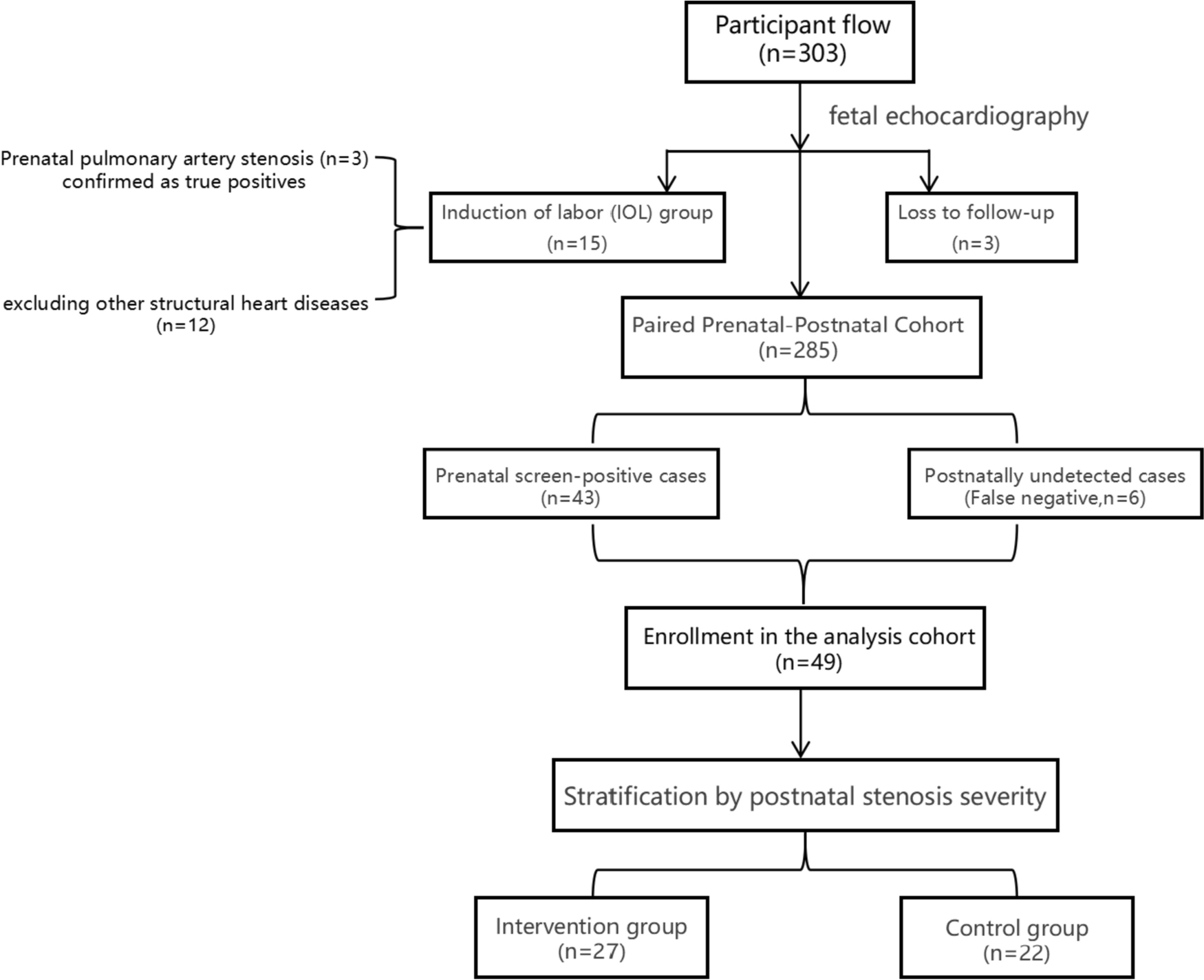
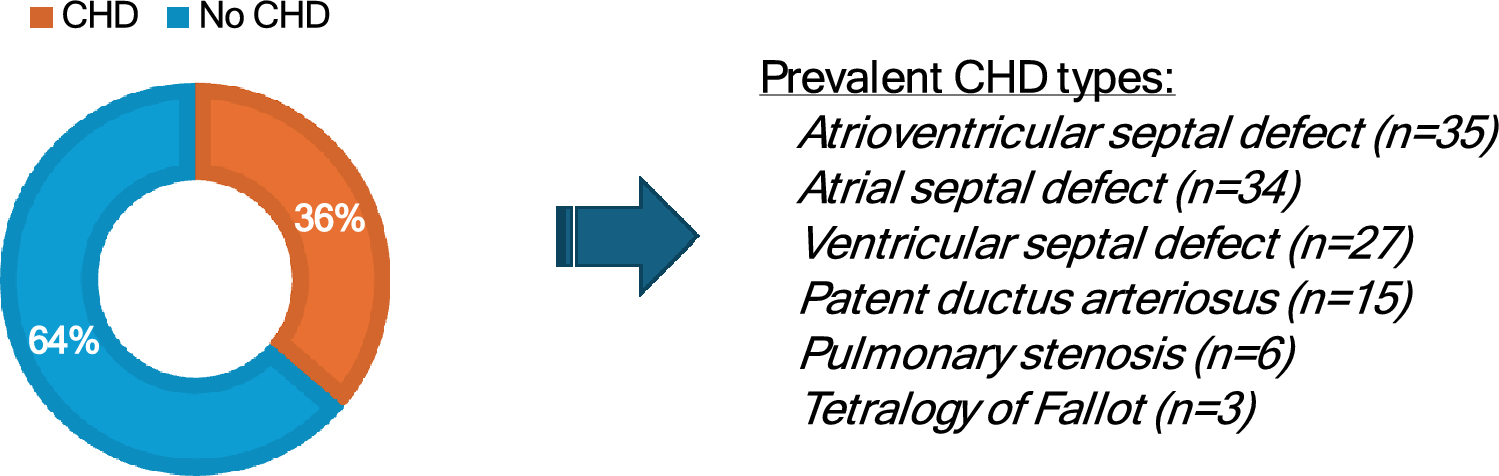
To evaluate prenatal echocardiography predictors of postnatal pulmonary stenosis (PS) requiring infant surgery. Consecutive fetuses with suspected cardiac anomalies (n = 303) were screened. After excluding cases of induced abortion (n = 18), the remaining cohort of 285 fetuses was analyzed. Postnatal follow-up confirmed PS in 30 neonates. Diagnostic consistency (kappa statistics) and risk factors (logistic regression/ROC analysis) for surgical intervention were assessed. This study enrolled fetuses with structurally abnormal hearts prenatally diagnosed with PS, defined by accelerated pulmonary forward flow (peak velocity > 1 m/s) concomitant with pulmonary valve abnormalities (thickening/increased echogenicity/restricted opening) or main pulmonary artery narrowing with post-stenotic dilation. Exclusions: ① PS with complex congenital heart disease (e.g., tetralogy of Fallot, ventricular septal defect, pulmonary atresia, transposition of great arteries); ② lost-to-follow-up/incomplete data; and ③ pregnancy terminations. The mean gestational age was 28.5 ± 4.91 weeks in the non-intervention group and 27.6 ± 3.13 weeks in the intervention group. Moderate prenatal–postnatal diagnostic agreement was observed (kappa = 0.609, P < 0.001). Key surgical predictors included severe tricuspid regurgitation (OR = 14.167), pulmonary valve abnormalities (OR = 11.250), elevated flow velocity (≥ 1.85 m/s; OR = 3.939), and reduced PA/Ao ratio (≤ 1.415; OR = 0.005, all P < 0.05). Combined indicators demonstrated high predictive accuracy (AUC = 0.934). Pulmonary valve abnormalities showed 94.7% sensitivity; flow velocity ≥ 1.85 m/s yielded 73.7% sensitivity and 91.3% specificity. Prenatal echocardiography effectively stratifies PS severity and surgical needs. Critical markers (valve anomalies, flow velocity ≥ 1.85 m/s, PA/Ao ≤ 1.415, severe regurgitation) optimize risk prediction, guiding clinical management.

Comments (0)