
Remember me
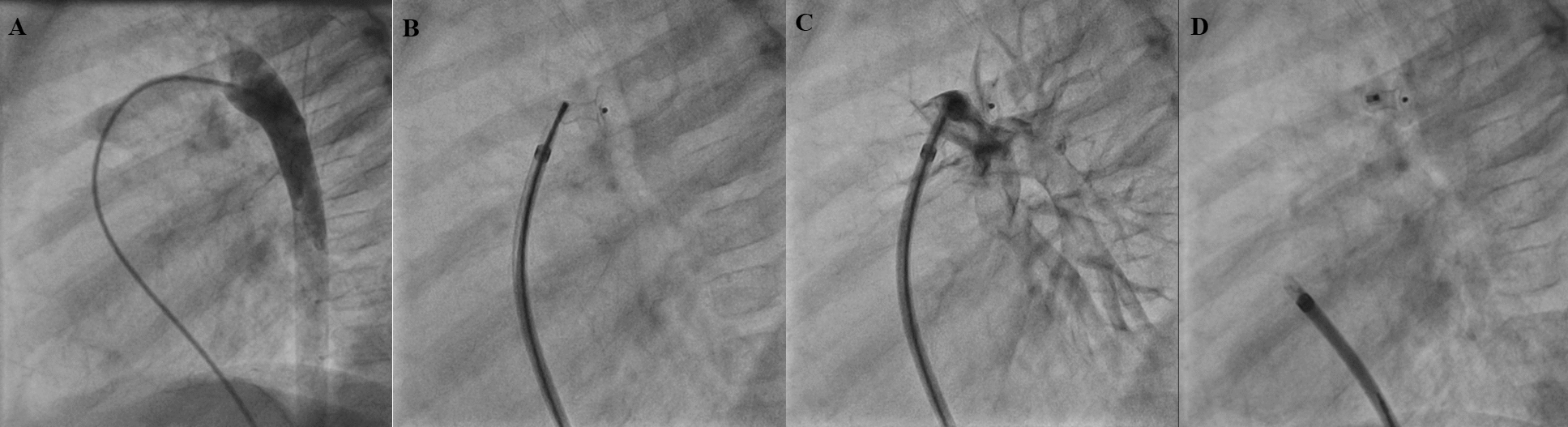
This case involves a one-year-old female patient with a history of Down syndrome. At presentation, her weight was 9 kg and her height was 65 cm. Her underlying cardiac anatomy included a balanced complete AV septal defect (Rastelli type A) and a patent ductus arteriosus. At one month of age, she underwent ductus arteriosus ligation and pulmonary banding due to pulmonary overcirculation. At 9 months, she was admitted for surgical repair, which included pulmonary banding removal and complete AV septal defect correction using the two-patch technique. Intraoperatively, the right AV valve exhibited severe regurgitation. An attempt at valve plasty was unsuccessful, leading the surgical team to implant an EPIC SUPRA PLUS N19 bioprosthesis, which showed no leakage on the continence test. In the immediate postoperative period, the patient developed severe biventricular dysfunction, requiring central venoarterial extracorporeal membrane oxygenation (VA-ECMO) cannulation.
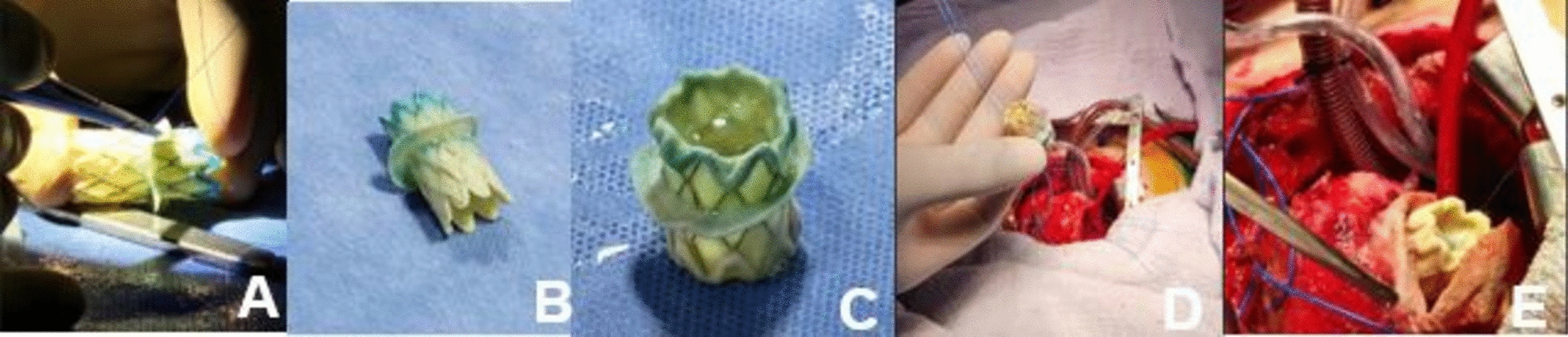
A Melody valve (22 mm) was successfully implanted in the right AV position as a palliative measure. The valve was expanded to a diameter of 14 mm using an XXL balloon inflated to 6 atmospheres and then secured to the valve annulus. Post-procedure, echocardiography confirmed adequate valve function with a 3-mmHg gradient.
Postoperatively, the patient remained dependent on VA-ECMO, with severe right ventricular dysfunction. Although right AV valve function was preserved, her condition remained unchanged. Given the lack of improvement, a joint decision was made with the family to withdraw VA-ECMO support, and the patient passed away the following day.
Case 2A two-year-old female patient. At presentation, her weight was 12 kg and her height was 69 cm. She had a history of Shone syndrome and, at seven days of life, had undergone successful repair of aortic coarctation and aortic arch reconstruction. At two years of age, she developed severe mitral regurgitation secondary to a perforation in the A2 segment of the anterior leaflet. She subsequently underwent mitral valve plasty and leaflet reconstruction. However, the intraoperative outcomes were poor, necessitating immediate support with central VA-ECMO. In the immediate postoperative period, echocardiography revealed persistent severe mitral valve regurgitation with significant hemodynamic compromise.
A 22-mm Melody valve was then successfully implanted in the mitral position as a palliative measure. The valve was expanded in the mitral position using a NuMED Canada Inc. Z-MED II™ 16 mm × 3 cm balloon, inflated to 6 atmospheres, and secured to the native mitral valve annulus. Transesophageal echocardiography immediately confirmed a mean gradient of 3 mmHg, with laminar flow and no obstruction of the left ventricular outflow tract (Fig. 3).
During three years of follow-up, the patient remained clinically stable, experiencing no complications or hospital readmissions and maintaining functional class I status. Serial echocardiographic evaluations consistently showed a normally functioning valve with a mean gradient of 5.5 mmHg (Fig. 2), without evidence of left atrial dilation or signs of pulmonary hypertension.
Fig. 2
Follow-up echocardiography 2 years after the procedure. A Apical 4 C Melody valve. B Apical 4 C in diastole with Melody valve with adequate leaflet closure. C Apical 4 C with color Doppler without evidence of significant flow acceleration, with a mean valvular gradient of 5.5 mmHg
Case 3A 6-month-old female patient. At presentation, her weight was 6 kg and her height was 59 cm. She had a history of severe mitral valve stenosis, critical coarctation of the aorta, and hypoplasia of the aorta. At 5 days of life, the patient was taken to aortic arch reconstruction, mitral valvuloplasty, and a calibrated 5-mm atrial septal defect. At 5 months, the patient presented to the emergency room with signs of heart failure and evidence of severe mitral valve stenosis and insufficiency on echocardiogram, with a maximum gradient of 21 mmHg and a mean gradient of 12.5 mmHg. The patient was admitted to the intensive care unit. The patient underwent the palliative placement of a modified 22-mm Melody valve in the mitral position. The valve was expanded to 16 mm using a Z-MED II™ balloon, inflated to 6 atmospheres. Immediate transesophageal echocardiography confirmed a mean gradient of 3 mmHg with laminar flow.
During follow-up, the patient was stable, with significant improvement in the signs of heart failure, and without stenosis and mitral valve insufficiency, which allowed dismantling of management for heart failure. Two years after the procedure, the patient was readmitted to the intensive care unit with ventilatory failure due to respiratory syncytial virus infection, which is why he died 2 years and 8 months after the procedure.
Case 4An eight-month-old male patient, weighing 6.9 kg and 61 cm in height at presentation, had a complex cardiac history. His underlying conditions included Tetralogy of Fallot with mild pulmonary stenosis, a mitral supravalvular membrane, moderate mitral regurgitation, a subaortic membrane, and aortic root dilation. He underwent surgical correction, which involved infundibulectomy, closure of the interventricular communication with a pericardial patch, mitral valvuloplasty, and resection of the subaortic membrane.
In the early postoperative period, echocardiography revealed a double mitral lesion, characterized by stenosis (mean gradient of 9 mmHg) and severe regurgitation, associated with biventricular dysfunction (severe right and moderate left). The patient’s initial postoperative course was complicated, requiring ventilatory and inotropic support, with no significant improvement observed during the first two weeks. Consequently, a 22-mm Melody valve was successfully implanted in the mitral position as a palliative measure. The valve was positioned at the mitral annulus without complications and dilated using a 16 × 40 mm XXL balloon at 5 atmospheres.
However, in the immediate postoperative period, the patient experienced an unfavorable outcome due to stenosis between the newly implanted Melody valve and the anterior leaflet of the native valve, resulting in a mean gradient of 10 mmHg and a superior paravalvular leak. Reoperation with anterior leaflet resection and repositioning was therefore performed. Intraoperative evaluation confirmed valve competence, and subsequent echocardiography showed adequate valve function, without residual stenosis or regurgitation, with a mean gradient of 5 mmHg.
The patient was discharged one month after the reoperation, with a Ross functional class II. He has been followed as an outpatient for eight-month post-procedure. Serial echocardiographic evaluations consistently showed a normally functioning valve with a mean gradient of 4.5 mmHg (Fig. 3), without evidence of left atrial dilation or signs of pulmonary hypertension.
Fig. 3
Follow-up echocardiography eight-month post-procedure. A Apical 4 C in systole with Melody valve with adequate opening. B Apical 4 C with color Doppler without evidence of significant flow acceleration, with a mean valvular gradient of 4.5 mmHg
Comments (0)