
Remember me
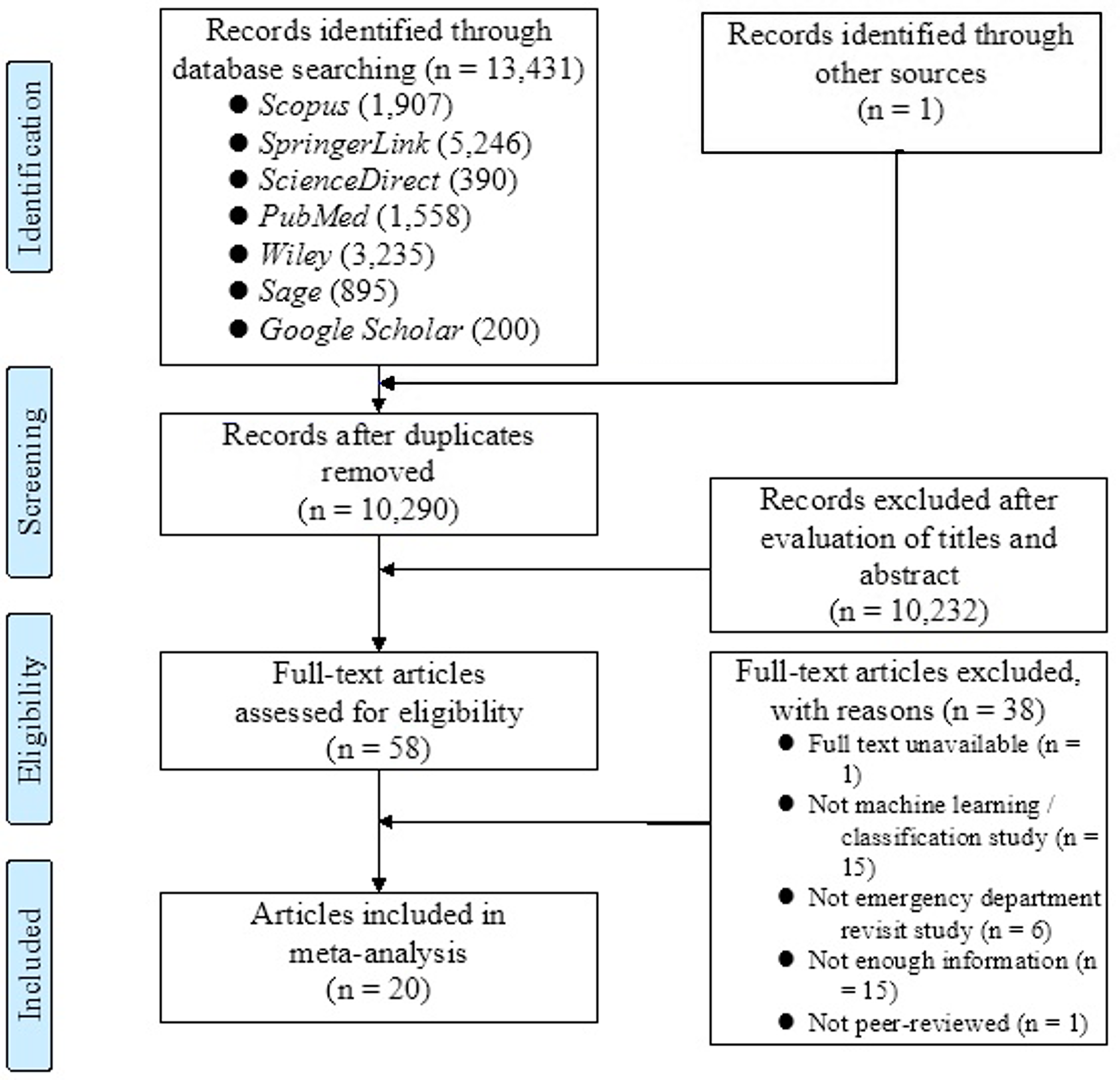
The search yielded 7830 items, from which 3022 duplicates were removed. Of the remaining 4801 articles, 4758 were deemed irrelevant to the scope of this review. Consequently, 43 papers were selected for full-text review. Following the application of inclusion criteria, 16 papers were included in the final analysis (Fig. 2). The results were conducted using the PICO framework, which also provided the reasons for excluding studies after full-text screening.
Fig. 2
PRISMA flow chart depicting the different phases of the systematic review
Study CharacteristicsThe included papers comprised the following study designs: Randomized Controlled Trials (RCTs) (n = 10) and Non-Randomized Controlled Trials (non-RCTs) (n = 6). The non-RCTs included one comparative study and five non-comparative studies. The study characteristics are summarized in Tables 2, 3, 4, 5, 6 and 7 in the appendix.
Table 2 Study characteristics (NRS = Non-randomized study; U = Understanding; S = Satisfaction; A = Anxiety; ↑ Increased; = No difference; ↓ Reduced)Description of the Patient PopulationA total of 1067 patients were included in this systematic review, with 32% being female and 68% being male. The low proportion of female participants is primarily due to the study by Wake et al. (10% women), which focused on prostate and kidney cancer, and studies by Hatzl et al. (12% women) and Grab et al. (13% women), which involved patients with vascular diseases [28, 37, 38].
The average age of patients from 14 of 16 studies is 57.4 years. Two studies reported patient age in ranges, excluding them from the average calculation. Castellanos et al. [25] reported 4% of patients aged 41–60 years and 96% over 61 years, while Chang et al. reported 6% aged 30–40 years, 15% aged 40–50 years, 24% aged 50–60 years, and 55% over 60 years [25, 26].
The systematic review includes studies from various specialties: cardiology (n = 6), neurosurgery (n = 5), organ transplant surgery (n = 2), vascular surgery (n = 1), plastic and reconstructive surgery (n = 1), and urology (n = 1) [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] (Table 2).
Used InterventionsFor the descriptive presentation of the results, the studies were divided into three categories based on the interventional visualization tool used: VR HMD (n = 12), AR HMD (n = 2), and MR HMD (n = 2) [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]. Details on the interventional visualization tools are presented in Tables 2, 3, 4, 5, 6, and 7.
Description of the Study OutcomesThis systematic review focuses on the impact of using different HMDs on patients’ understanding, satisfaction, and anxiety.
The term"patients’ understanding"encompasses various terms used in the included studies, such as"patient knowledge", “informational gain”, “procedural knowledge”, “patients comprehension” and “information desire” [27, 28, 31, 35, 38, 39]. For simplicity, all these outcomes are summarized as"patients’ understanding".
Patients’ satisfaction was measured directly with questionnaires in some studies, while others used additional terms such as “usability”, “effectiveness”, “self-efficacy”, “preferred patient education tool”, “comfort level”, “usefulness”, “happiness” and “Patient-Doctor Relationship” [24,25,26,27, 29, 30, 32, 33, 35,36,37,38,39]. For simplicity, all these outcomes are summarized as"patients’ satisfaction."
Objective outcomes were assessed using pre- and post-intervention questionnaires, and post-intervention questionnaires only.
Patients’ UnderstandingAmong the 16 studies using VR, AR, or MR HMDs in preoperative informed consent, 12 examined patients’ understanding. Of these, 8 studies utilized VR HMDs, two studies used AR HMDs, and two studies used MR HMDs [25,26,27,28, 31, 32, 34,35,36,37,38,39].
All 8 studies employing VR HMDs reported positive effects on patients’ understanding. Four non-randomized, non-comparative studies indicated improved patients’ understanding, with Wright et al. demonstrating statistically significant improvement in patients undergoing elective craniotomy [32]. The other three studies reported an improved understanding with no information of statistical significance in 98% of participating patients with cardiac interventions, in anatomic understanding of kidney patients, and in 97% of participating patients about their upcoming atrial fibrillation ablation procedures [25, 27, 34].
Four RCTs evaluated the impact of VR HMDs compared to standard educational methods including 2D images, verbal education, and paper education [26, 28, 31, 35]. In the study by Grab et al., patients were divided into three groups: one receiving VR-HMD-based education about their cardiac surgery, another using 3D printed models, and a control group. The VR-HMD group demonstrated the most significant statistical improvement in understanding their medical condition after informed consent [28]. Perin et al. also included two intervention groups, one using VR-HMDs for brain tumor visualization and the other utilizing a 3D screen. Patients in the VR-HMD group exhibited the highest level of understanding, significantly surpassing the control group [31]. Kwon et al. found that patients educated with VR-HMDs had a significantly lower information desire regarding their plastic or reconstructive surgery compared to the control group, indicating a better understanding of their condition and the procedure [35]. Additionally, Chang et al. reported that patients undergoing catheter ablation for atrial fibrillation who received VR-HMD education showed improved pre-procedure knowledge compared to those in the control group [26].
Among the two studies that examined patients’ understanding using AR HMDs, the results differ. In the non-randomized non-comparative study by Lee et al., all patients reported a statistically significant improved understanding of their medical condition using AR HMDs, whereas Wake et al. found no improvement compared to 2D imaging used in the control group in their RCT [36, 37]. In the study by Wake et al., patients’ understanding was additionally examined by using 3D printed models and visualization as 3D computer models in further intervention groups. The use of 3D printed models significantly improved patients’ understanding. The 3D computer model also performed significantly better as an intervention group than the AR HMD compared to the control group [37].
Studies utilizing MR HMDs generated mixed results. Notably, the variation in control group visualization methods between the two studies limits their comparability. In an RCT by Hatzl et al., the use of MR HMDs during preoperative informed consent was compared with 2D images displayed on a monitor. Both groups exhibited improved patients’ understanding compared to the pretest, but no significant difference was found between the two groups [38]. In contrast, House et al. compared MR HMDs with a rubber brain model, demonstrating that patients’ understanding was statistically significant higher when using the MR HMD compared to the rubber brain model (Fig. 3) [39]. Additional detailed information can be found in Tables 3, 4, 5, 6, 7, and 8 in the appendix.
Fig. 3
Patients’ understanding of their disease after the informed consent consultation using a VR, AR, or MR HMD compared to the control group (Improvement, statistically significant (N = 6): [28, 31, 32, 35, 36,
Comments (0)