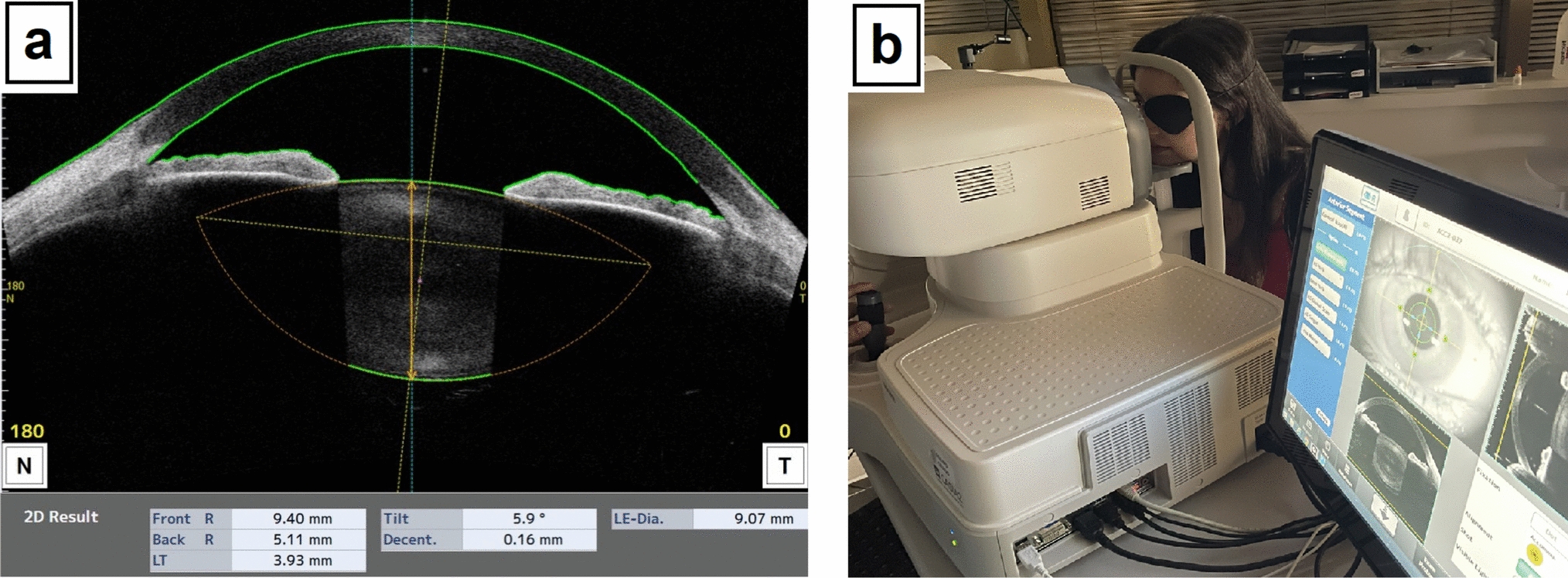
Fourier harmonic analysis of the corneal surface demonstrated that regular and irregular corneal astigmatism was significantly higher in the LSCD group than in the control group. An increase in irregular astigmatism, which is challenging to correct with spectacles, was observed in the early stages of LSCD, and higher-order irregularity increased significantly in stages II and III, suggesting that irregular corneal astigmatism tended to worsen as LSCD progressed. This may have been caused by irregular epithelial thickness, stromal thinning, peripheral neovascularization of the cornea, corneal epithelial defects, and corneal scarring. In the corneas of patients with LSCD, the conjunctiva gradually invades from the periphery to the central cornea. The conjunctiva subsequently invades the pupil in stages II and III of LSCD, blocking the passage of light and leading to vision impairment. In contrast, in stage I of LSCD, the invading conjunctiva does not cover the transparent central cornea but changes the three-dimensional structure of the corneal shape with pulling power. The same phenomenon has been observed in cases of pterygium, where the conjunctiva extends into the cornea, similar to the events in LSCD, resulting in an increase in corneal irregularity with disease progression [15]. Conjunctivae that extend close to the pupil are reported to alter the shape of the cornea even if they are not directly attached [16]. Furthermore, LSCD affected the anterior corneal surface, and topographic changes were observed on the posterior surface, as presented in Table 2. The posterior surface of the cornea, the endothelial cell layer, is not directly invaded via neovascularization owing to the loss of function of limbal stem cells. Fig. 5a and b illustrate a representative case of LSCD with evidence from both the anterior and posterior surfaces. The tomography results in Fig. 5a show corneal thinning and protrusion similar to keratoconus, while the posterior Fourier index map in Fig. 5b shows anterior protrusion of the posterior corneal surface and increased posterior regular astigmatism, asymmetry, and higher-order irregularity. Based on these observations, we suggest that the progression of the conjunctiva onto the cornea on the anterior surface distorts the entire cornea and that its effects extend to the posterior surface of the cornea.
Our clinical study demonstrates that greater irregular corneal astigmatism, especially higher-order irregularity, explains the low visual acuity in patients with LSCD. It is challenging to evaluate corneal astigmatism because the mire ring in keratometry is distorted in patients with rough ocular surfaces. Here, the newly developed AS-OCT enabled us to evaluate the corneal topography in the central 3-mm diameter of the anterior and posterior cornea. Previously, Ibrahim et al. reported that high-order aberrations correlated highly with visual acuity in patients with SJS and TEN [17]. However, there is no detailed information regarding corneal anterior and posterior astigmatism in patients with LSCD. Moreover, several patients with LSCD also have corneal opacity due to primary diseases (SJS/TEN, OCP, or chemical burns), because higher-order aberrations are sometimes affected by corneal opacity. Therefore, we focused on assessing corneal refractive characteristics using Fourier harmonic analysis. Fourier analysis provides a more detailed assessment of corneal shape, including spherical components, regular astigmatism, asymmetry components, and higher-order irregularity. Both Fourier analysis and Zernike polynomials are valid methods for analyzing corneal shape, and both corneal analysis techniques are clinically useful. In the current research, we chose Fourier analysis for the following reasons: (1) Fourier analysis enables us to decompose the corneal shape comprehensively, breaking down the corneal surface into four parameters in a form that clinical ophthalmologists can easily understand; (2) Fourier analysis is correlated with visual outcomes: spherical components and regular astigmatism can be corrected with spectacles, whereas asymmetry components and higher-order irregularity cannot and require correction using contact lenses. This distinction is important for patients, as understanding whether they need glasses or contact lenses is clinically valuable. Based on the results of Fourier analysis, ophthalmologists can select and prescribe the appropriate visual aids; Furthermore, Fourier analysis allows for the classification of the causes of irregular astigmatism, distinguishing whether they result from asymmetry or higher-order irregularity, making the interpretation more intuitive. (3) Fourier components can be displayed as color-coded maps, facilitating easier interpretation of corneal shape characteristics for both doctors and patients. At the same time, it is also important to understand aberrations by Zernike polynomials, as they allow for a detailed classification of optical distortions, including coma and trefoil, and provide a standardized approach to wavefront analysis. Further analysis for patients with LSCD is needed in the future to better characterize the optical impact of corneal irregularities.
In this study, only higher-order irregularity was correlated with visual acuity. However, it seemed likely that asymmetry components would be associated with visual acuity because these components are not corrected with spectacles. In the present study, Fig. 2c shows a tendency for visual acuity to worsen as asymmetry components in the anterior cornea increased, although this was not significant (P = 0.083). In Fig. 3c, P = 0.067 was not significant either, but there was a tendency for visual acuity to worsen as the asymmetry components of the posterior corneal surface increased. Since the number of patients in this retrospective observational study was only 25, and the ocular surface shape of LSCD patients is highly variable, further studies with a larger number of patients are needed.
Treatment for irregular astigmatism not corrected by spectacles is limited. Although RGP lenses generally provide better outcomes for patients with high corneal astigmatism, they cause mechanical trauma, dry eye, hypoxia, and preservative toxicity that lead to stress in the corneal epithelial cells and can induce LSCD; therefore, RGP lenses should be avoided [5, 18, 19]. Alternatively, scleral lenses have been developed to retain fluid on the irregular surface of the cornea and maintain visual acuity [20, 21]. Correction of irregular corneal astigmatism improves visual acuity in the scleral lens, but the scleral lens causes hypoxia on the ocular surface, possibly leading to the progression of LSCD [21]. Therefore, these lenses should be used cautiously, with the degree of progression being observed frequently. Cultivated limbal epithelial cell sheet transplantation, another treatment option in regenerative medicine, was developed to reconstruct the ocular surface [22]. Despite these advances, it would be desirable if LSCD progression could be stopped before reaching a stage where the irregular astigmatism becomes more marked. Furthermore, once treatment for advanced cases is established, there is potential for improvement in corneal irregularity, leading to better visual acuity.
The current study had some limitations. First, cataracts and macular hypoplasia were often noted in patients with aniridia, and there was a significant difference in BCVA between the LSCD and control groups. However, sex, age, and central corneal thickness showed no intragroup differences. Therefore, we only analyzed the relationship between the four components of the Fourier harmonic analysis and BCVA in the LSCD group. Second, patients with SJS/TEN or OCP sometimes have symblepharon, which attaches to the conjunctiva near the cornea and the eyelids and can affect corneal topography. To account for this issue, we carefully examined the patients' eyes and applied as little extra pressure as possible to the eyeball after opening the eyelids. Third, in the present study, we were unable to determine which corneal factors—epithelium or stroma—have the greatest influence on corneal irregular astigmatism, as we could not accurately assess epithelial and stromal thickness using anterior segment optical coherence tomography. Fourth, visual function is influenced by both astigmatism related to corneal shape and reduced corneal transparency. Although we could not evaluate the degree of corneal opacity in this study, it is possible that it affected visual acuity. Since AS-OCT can evaluate densitometry, future studies should consider densitometry values according to LSCD staging.
In conclusion, an increase in irregular astigmatism was observed on both the anterior and posterior corneal surfaces in patients with LSCD, regardless of the stage, using Fourier harmonic analysis of AS-OCT.

Comments (0)