In the present study, surgical correction for de novo AI was indicated for patients with more advanced heart failure than in previous studies. Grinstein et al. [18] reported that right heart catheterization results varied widely according to the severity of AI in patients with LVADs, with pulmonary artery wedge pressures of 10.2 mmHg in the no-AI group and 15 mmHg in the moderate or higher group. In the current study, the patients showed pulmonary artery wedge pressures of 19 mmHg after development of de novo AI, which indicates apparently advanced heart failure compared with previous reports. However, surgical correction of de novo AI was safely done in all patients and significant improvement in hemodynamic parameters such as pulmonary capillary wedge pressure was confirmed.
When prosthetic valve replacement is performed in non-LVAD patients with chronic AI, left ventricular reverse remodeling and hemodynamic improvement often take up to 6 months. [19] In chronic AI, the left ventricle is capacitively loaded for a reasonable time before surgery is indicated and remodeling progresses. In contrast, the patients with LVAD have end-stage heart failure as a result of cardiomyopathy or myocardial infarction, and their cardiac function is severely impaired as a result of progressive cardiac remodeling. De novo AI after LVAD implantation cannot compensate for the increased volume load caused by the blood ejected by the LVAD returning into the left ventricle and this leads to heart failure. Staving off this “re-circulation” restores the efficiency of the LVAD and results in an immediate hemodynamic improvement. In other words, in terms of left heart parameters (PCWP, CI and SvO2), physical improvement of AI may have improved early postoperative hemodynamics by allowing enough unloading of LV and enough output to systemic circulation in patients dependent on LVAD. In addition, based on the values of right heart parameters (CVP, PAPi and RVSWI), early surgical intervention for aortic valve before right heart failure progressed may have led to a good outcome.
As for a technique of surgical correction of AI, Park’s stitch is a simple and widely used especially for de novo AI management in LVAD patients [15] but recurrence after long-term follow-up has been reported [20, 21]. To achieve complete control of AI, we used patch closure of the valve despite it requires a slightly longer cardiac arrest time. [22]
Overall, the postoperative survival rates after surgical intervention for AI in patients with LVAD in this study seems better compared with those reported in previous studies. Adamson et al. [16] performed aortic valve closure in 28 patients and reported a 1-year survival rate of 78% and a 3-year survival rate of 53%. Rao et al. [17] performed surgical intervention for aortic valve in seven patients, with a 1-year survival rate of 71.4%. Yehya et al. [23] performed transcatheter aortic valve implantation in nine patients and reported a 1-year survival rate of 56%, while Phan et al. [24] performed transcatheter aortic valve implantation or percutaneous occlusion device therapy on 29 patients and reported an in-hospital mortality rate of 31%. Transcatheter aortic valve implantation and percutaneous occlusion device therapy may be advantageous in terms of surgical invasiveness. However, off-label use and serious complications have been reported; therefore, the percutaneous treatment of de novo AI requires careful consideration. Aortic valve closure or replacement via re-sternotomy may be a reasonable therapeutic approach when AI in patients with LVADs can no longer be managed conservatively.
Our study has several limitations. As a single-center study, the sample size was small. However, no previous studies on de novo AI after LVAD implantation requiring surgical intervention involving large samples have been reported. Few reports of hemodynamic improvement after aortic valve repair via re-sternotomy in patients with severe de novo AI after LVAD implantation or of outcomes in such patients are available. The novelty of this study lies in the analysis of hemodynamics before and after intervention for aortic valve in this patient population. Our report provides valuable information on these issues despite the small sample size. Additionally, quantitative assessment of AI severity after LVAD placement is difficult, and no consensus method is currently available. Finally, long-term follow-up data to assess long-term outcomes were lacking.
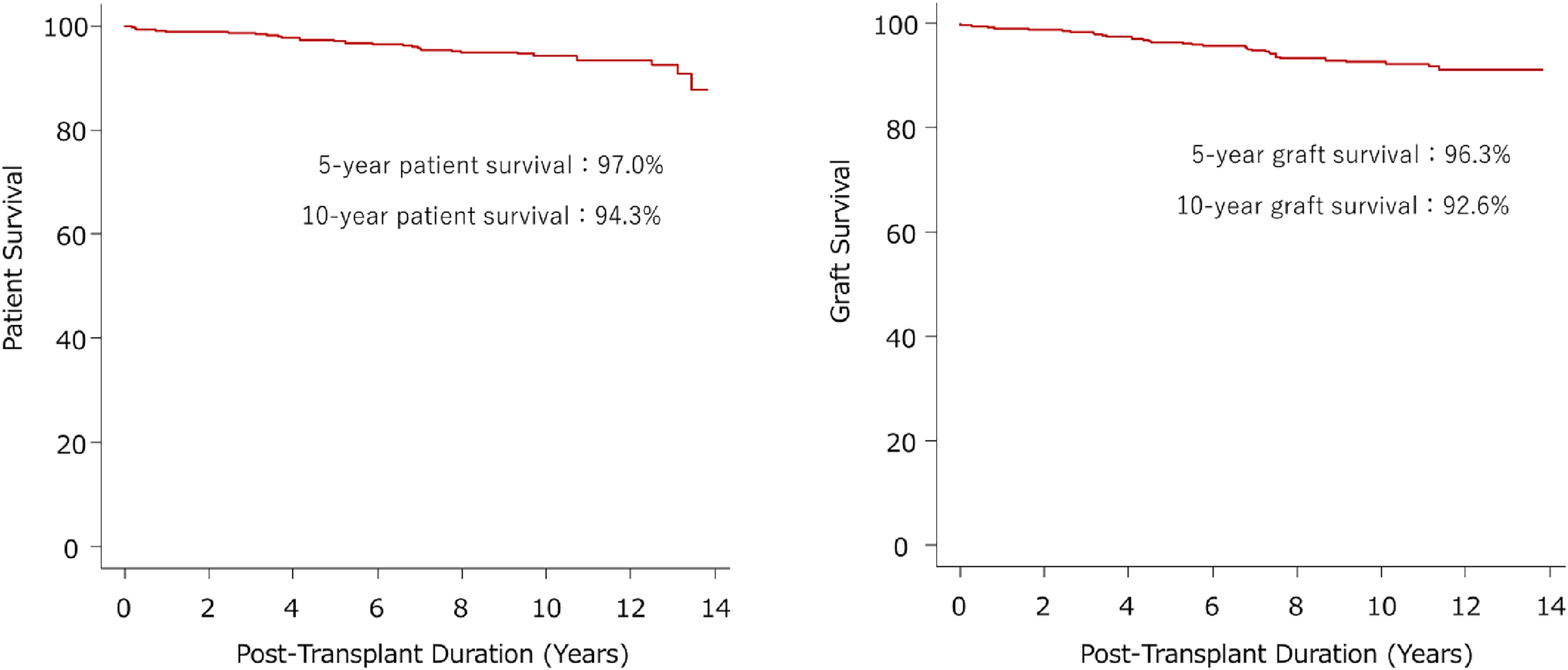
In conclusion, our findings suggest that postoperative hemodynamic status and survival rates are favorable in patients who underwent aortic valve closure or replacement for de novo AI after LVAD implantation.

Comments (0)