1) Description of selected studies
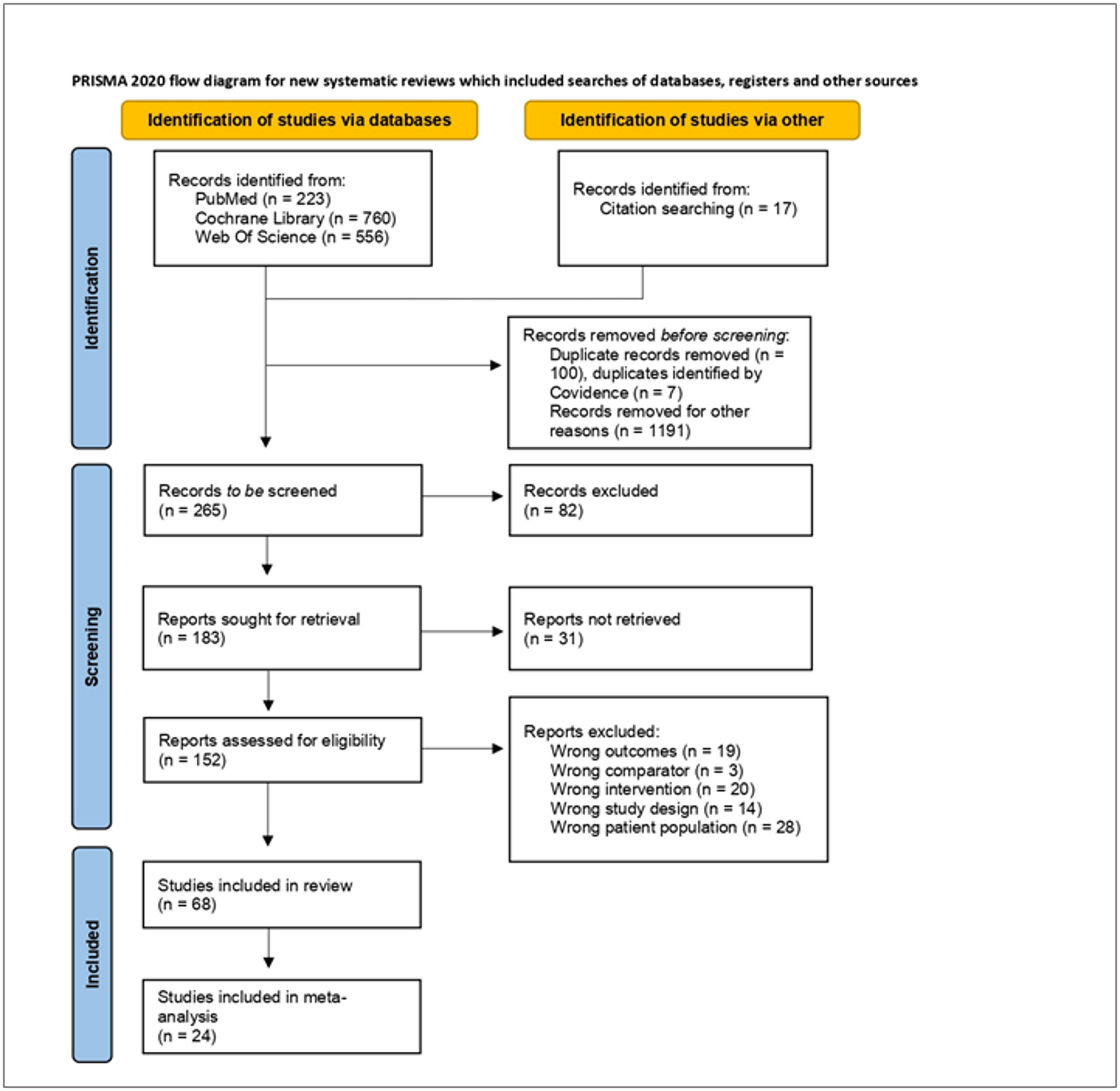
The search strategy identified 4246 citations, including 84 protocols for interventions using a participatory approach. These 84 protocols were not considered for further review. Titles and abstracts were screened for meeting the inclusion criteria, yielding 36 articles. A further 12 papers were added through hand searching. Full texts were retrieved from this total set and another 36 were excluded for not meeting the inclusion criteria upon analysis of the full article, leading to a final set of 12 studies as shown from the PRISMA in Fig. 1. Mayer et al. (2019) was not found in the initial search, as this paper builds on the participatory process applied in the pilot project that was described by Parikh et al. (2010) [26, 27]. The study by Nollen et al. (2014) was preceded by an earlier paper (2013), however this earlier paper was not included as the study focused on feasibility testing of the intervention without describing impact, and did thus not meet our selection criteria [28, 29].
Included studies were published between 2008 and 2019. Nine out of 12 studies were from the United States, with single studies from Australia, Canada and India (Tables 1 and 2). Table 1 presents further characteristics of the interventions. The interventions were mostly directed towards individuals (Balagopal et al., 2012, Davison et al., 2013, Cherrington et al., 2013, Goldfinger et al., 2008, Nollen et al., 2014, Parikh et al., 2010, Reifsnider et al., 2018, Sendall et al., 2016), while one applied a systems approach that was aimed at the community (Liao et al., 2016) and two interventions targeted both the community and individuals (Wright et al., 2013, Ziabaksh et al., 2016) [27, 28, 30,31,32,33,34,35,36,37,38].
Below we review how the included studies made use of theory, participation and how studies were evaluated. Furthermore, the extent of participation, who participated and what approaches were used in the formative, implementation, evaluation, and feedback phase of the interventions is described in order to further classify the included studies and identify common learnings.
Table 2 Description of studiesUse of theory
Seven interventions were theory-based. Five of them applied theories from social psychology: self-efficacy (Parikh et al., 2010; Mayer et al., 2019) / self-determination theory (Cherrington et al., 2015)/ the principles of behavioural weight control (Nollen et al., 2014); the family ecological model (FEM) - a family centered developmental theory that emphasizes the context as a shaping factor for family behaviour - as well as empowerment theory a framework aimed at enhancing self-determination of individuals and communities (Davison et al., 2013) [26,27,28, 31, 32]. In the FEM, caregiving practices and family daily living strategies are shaped by factors that are proximal to families in combination with their broader contexts. Nollen et al., (2013,2014) applied grounded theory, a theory that derives concepts from the data and develops them by collecting, coding and analysing data concurrently [28, 29]. Finally, Ziabakhsh et al. (2016) applied feminist theory [38].
Use of participatory protocol
Studies used a range of protocols for their participatory research. Of the 12 studies selected, seven used community-based participatory research (CBPR) [26, 27, 30, 31, 33, 36, 37] using the guidelines for such research as described by Peters et al. (2015) [21]; two studies in Latino communities in the USA involved promotora’s, i.e. community members without formal healthcare education but often with specialized training to liaise between communities and health and social service providers [32, 34]; two studies applied a community-engaged approach [28, 38]) and one study applied PAR (participatory action research [35]).
Studies claiming to apply CBPR without detailing its implementation entirely were excluded during the screening process.
Study assessment design
The study design included a control group in half of the studies ( [26,27,28, 30, 34, 36, 37] and this was by means of an RCT in all but two of these studies. In contrast, a pre-post design was applied in the remainder of the quantitative evaluations, and Ziabaksh’set al., (2016 [38]), evaluation was based on subjective assessment of health.
Level of evaluation
The group of interventions targeted at the individual included health education messages, courses and workshops that mostly addressed nutrition, physical activity and stress management that were culturally sensitive (Table 3). In contrast, the REACH US project took a systems approach where they targeted the “upstream” causes of health disparities in communities [36]. REACH US was launched in 2007 by the Centers for Disease Control and Prevention. Through environmental and system improvements the project facilitated healthy eating and active living by making such choices easier, more convenient, affordable, safe and a behaviour norm. This intervention stands out for its approach, its scale (14 Black communities in 10 US states), and for the duration of the evaluation (4 years of monitoring). In all these communities, the interventions were focusing on: building strong community-based coalitions; focusing on policy, systems and environmental improvements; and culturally tailored interventions. Of the two studies targeting both communities and individuals, Wright et al. (2013) provided weekly physical activity and nutrition education through a school-based programme (Kids N Fitness©) for parents and children [37]. This programme was embedded into a more integral approach and intervention sites also participated in school-wide wellness activities, including health and counseling services, staff professional development in health promotion, parental education newsletters, and wellness policies for the provision of healthy foods at the school. The second intervention targeting communities and individuals by Ziabaksh et al. (2016) aimed at reducing risk factors for cardiovascular diseases and the intervention evolved over time [38]. In their study, initially, nurse practitioners felt strongly about goal setting as a separate component of the intervention but during the intervention the Talking Circle became the backbone of the intervention into which goal setting was embedded in a culturally sensitive and appropriate way [38]. Health messages were adopted to spiritual practices of the community. For example, smoking could not simply be a risk factor as “holy smoke” is part of healing practices in the community.
Table 3 Study characteristics2) Extent of participation in intervention
To further specify the extent of participation, we ranked the selected papers based on their participative elements in the formative, implementation, evaluation, and feedback phase of the research project and categorised them into two groups. Table 4 presents participation in each of the phases of research. The first group includes studies that are participative in all phases of the research (identified as fully participatory in Table 4), while the second group is participative in only some of the phases or lacks a detailed description of the nature of the participation (identified as participatory in Table 4). For example, some studies in the second category described co-creation for the planning and execution phase, yet no clear description of collaboration in other phases such as the design was evident.
Table 4 Participants in various phases of selected studiesNext, the four phases of the intervention of the identified studies are described. More specifically, the partnerships that were established as well as the methods through which these partnerships were built in the formative phase are presented; this is followed by the elements of the intervention used in the implementation phase, and the study design applied in the evaluation phase as well as impact achieved; lastly, the reflection phase describes how the learning from the process as well as the evaluation were used to continue after the intervention was finished. Table 3 describes the participants included in the various phases, while Table 4 presents the methods used.
The formative phase of the research includes the development of the intervention. Studies built the development of their interventions on engagement with different partnerships, such as a collaborative or community academic partnership or coalition [26, 27, 30, 33, 37]), a (community) advisory board (CAB) [28, 31, 32, 34]) and community leader-led [38]. Table 4 presents the participants of each of those coalitions/ partnerships/ advisory boards in the formative phase. The study by Wright et al. (2013) deserves some special mention [37]. Although the partnership between university of California and the underserved community was established over an 8 year period, the Kids N Fitness lifestyle intervention programme was developed previously by a university professor; only the lifestyle intervention was developed with CAB and implemented involving the School Advisory Health Council. Thus, only the environmental component of the intervention can be considered participatory.
In the implementation phase the participants include the change agents that would be leading the implementation of the intervention, for example parents in the case of studies in children [31] or CHWs [30], or community leaders (for example [36]), or promotoras [32, 34] or a subcommittee of the partnerships/ coalitions [27, 33]. The elements of the intervention were depending on the aim of the intervention and are presented in Table 5. This could for example include physical encounters, recipe contests, health education campaigns or Ayurvedic teaching. Such activities could be geared towards improved nutrition outcomes, physical activity, wellbeing, but could also include social or environmental elements.
Table 5 Methods & elements used across stages of selected studiesParticipants in the evaluation phase include the target population as well as those who did the assessments, although most studies did not specify the latter. Impact of the interventions was assessed based on individual-level or community-level indicators. The individual-level interventions used outcome indicators in the physical domain, such as anthropometric indicators, blood pressure, fasting glucose but also behavioural indicators such as dietary intake or food practices, knowledge scores and attitudes. Most studies described above used quantitative measures to assess impact. In contrast, in an indigenous population in Canada, Ziabaksh et al. (2016) applied a qualitative approach and focused on small steps achieved on dietary patterns, physical activity, and emotional as well as spiritual health [38]. The large-scale study by Liao et al. (2016) was evaluated based on the assessment of prevalence of obesity in the REACH US populations as compared to propensity matched controls from the Behavioural Risk Factor Surveillance System [36]. Interestingly, almost all studies described a positive effect of the intervention on the outcome indicators, and Davison et al. even found a dose-response effect of the intervention [31]. Only the interventions directed at parents of infants by Reifsnider et al. (2018) did not show an effect on outcome indicators, including overweight/ obesity status at age 12 months [34]. Nollen et al. (2014) observed only trends towards increased food and vegetable consumption as well as decreased sugar-sweetened beverage consumption of girls in a mobile device intervention [28]. In contrast, the school-based study by Wright et al., (2013) demonstrated a difference in effect on BMI reduction between boys and girls and pointed towards the importance of a gendered approach to prevent health disparities (Table 4) [37].
The final reflection phase of the interventions distinguished the two categories (highly participatory and participatory together with the formative phase. The reflection phase involved a reflective meeting, focus groups or a survey with the target population and/ or with the change agents and/ or coalition.
Examples of studies with full participation throughout the research project
To further illustrate the nature of the participation, two studies from the first category are described.
Davison et al., (2013) aimed to reduce childhood obesity together with families in upstate New York during a one-year multifactorial family-centered intervention [31]. The Family Ecological Model and Empowerment theory were used as theoretical underpinnings for the development of the intervention. Parents played an active and equal role in community assessment and using the findings to design a family-centered childhood obesity intervention. Parents also played a leading role in implementing the intervention and worked with the research team to evaluate the findings. The intervention included a poster campaign, BMI feedback letters and counseling sessions for parents as well as a program aimed at the children. A pre-post design at baseline and after a year was applied for evaluation [31].
The only qualitative study identified, concerns the development of a women-centered and culturally responsive heart health promotion programme among indigenous women in Canada by Ziabakshsh et al. (2016) [38]. The Seven Sisters intervention was informed by indigenous healing perspectives, transcultural nursing, and feminist theories of health and illness. This project engaged indigenous women leaders and Elders as champions of heart health who would simultaneously learn about and try to improve their own personal risk factors while contributing to shaping the healthy living practices of their community members. This approach reflects the indigenous value that wisdom comes from Elders and leaders. The Talking Circle that initially had been included as a minor part of the intervention, became more and more relevant in the course of the programme and other items, such as goal setting were eventually embedded into the culturally accepted Talking Circle. Evaluation involved analysis of the Talking Circle’s contents, a focus group, field observations, and self-completed surveys.
3. Impact of the interventions
Although a scoping review is not designed to evaluate (the direction of) impact, the selected studies broadly show positive outcomes in BMI/obesity reduction and other health indicators, across all fully participatory studies with quantitative approaches, independently of the demographics of the study populations (Table 6). Most notably, Mayer et al. (2019) and Liao et al. (2016) [26, 36] both showed a marked reduction in body weight and obesity respectively in relation to their established control groups, which is significant due to both the design and participant number in these studies, especially in the latter. Results in the studies with a lower level of participation were more mixed, and two of the four studies (Nollen et al., 2014 and Reifsnider et al., 2018 [28, 34]), showed no significant improvements in the measured parameters. However, the added value of a participatory approach should not be extrapolated from these results alone, as the studies herein differ significantly in aim, design and population demographics. Direct comparisons between each intervention and suitably-matched study would be required for adequate impact assessment.
Table 6 Study design, outcome measures and impact 
Comments (0)