
Remember me

To the best of our knowledge, this is the first study reporting on the impact of CRT on pre-existing hydronephrosis, evaluating the incidence and drainage of hydronephrosis following CRT. The findings reveal that pre-existing hydronephrosis in our cohort persisted in 74% (20/27) of the patients, with 44% (12/27) of the patients with persistent hydronephrosis ultimately receiveing drainage. Additionally, 21% (25/119) of the patients without pre-existing hydronephrosis developed hydronephrosis after CRT. Of these patients, 52% (13/25) underwent some form of drainage. In total, 17% (25/146) of patients treated with CRT received drainage.
The literature reports an incidence of hydronephrosis prior to CRT of 10-45% [7, 14,15,16,17]. This variability likely reflects a bias in treatment selection (RC vs. TMT), which can be attributed to the perceived eligibility of patients for CRT in the case of hydronephrosis. The incidence of hydronephrosis before CRT in our cohort (18%) is consistent with the literature. In 1631 patients undergoing RC an incidence of hydronephrosis of 25% before and of 38% after RC was reported, with a median follow-up of survivors of 10.5 years [18]. This is in line with our finding of an incidence of 31% (45/146) after CRT. Another retrospective study by Tanaka et al. reported hydronephrosis after RC in 11.4% (out of 290) patients after a median follow-up of 59.5 months [19]. This difference may be caused by the exclusion of pre-existing hydronephrosis by Tanaka et al. Nevertheless, we found hydronephrosis after CRT in 21% of patients without pre-existing hydronephrosis. Other studies only assessed the development of symptomatic anastomotic strictures requiring drainage after RC, reporting incidences of 3.4–16.8% [20,21,22,23,24,25]. However, there is a paucity of literature on the specific effects of RC on pre-existing hydronephrosis.
The present study demonstrated that pre-existing hydronephrosis was attributable to tumour in 93% (25/27) of cases. Hydronephrosis after CRT in patients without pre-existing hydronephrosis was caused by a tumour in 44% (11/25). In line with this, visual complete resection was significantly associated with hydronephrosis in these patients, as this is associated with larger tumour size, a higher risk of tumour progression and a higher risk of tumour recurrence [26, 27]. Interestingly, tumour location at the ureteral orifice was not associated with the development of hydronephrosis in these patients, possibly because recurrences can occur distant from the original site. In patients without pre-existing hydronephrosis where the tumour was not the cause of hydronephrosis after CRT, we hypothesize that the hydronephrosis is caused by thickening of the bladder wall or radiation-induced fibrosis with subsequent lack of stretchability, resulting in pressure on the ureters. The thickening of the bladder wall may be attributable to bladder wall hypertrophy, inflammation (acute) or fibrosis (chronic) resulting from CRT. Given the variability in the reaction of bladder tissue to CRT among individuals, this may consequently lead to unilateral and bilateral hydronephrosis.
In contrast, in only 22% of patients with pre-existing hydronephrosis tumour was responsible for remaining hydronephrosis after CRT. Possibly radiation-induced fibrosis may be a more important factor in this group. However, a challenge persists in distinguishing between fibrosis and persistent tumour due to the similarity of fibrosis and tumour in terms of imaging characteristics, namely thickening of the bladder or ureteric wall. Additionally, the limitation of cystoscopy in assessing tumour persistence in deeper layers must be considered. Nevertheless, it is important to note that each of these situations necessitates a distinct approach. In cases of fibrosis, treatment is directed towards preserving kidney function and managing symptoms. In cases of tumour persistence, additional radical treatment is indicated when feasible. This imposes a challenge for healthcare professionals.
Furthermore, a baseline eGFR < 60 ml/min/173m2, although not statistically significant (p = 0.063), was associated with an increased risk of hydronephrosis post-CRT with an HR of 2.89. No causal association exists between a decreased baseline eGFR and the development of hydronephrosis, thus there must be an unidentified confounder that causes this association. Possible confounders are cardiovascular disease and tumour size. Cardiovascular disease is included as a stratified variable, yet it could be underreported in our dataset. Tumour size, on the other hand, might also be the confounder since larger tumours may more often require NSAID and opioid analgetics, impacting eGFR [28, 29].
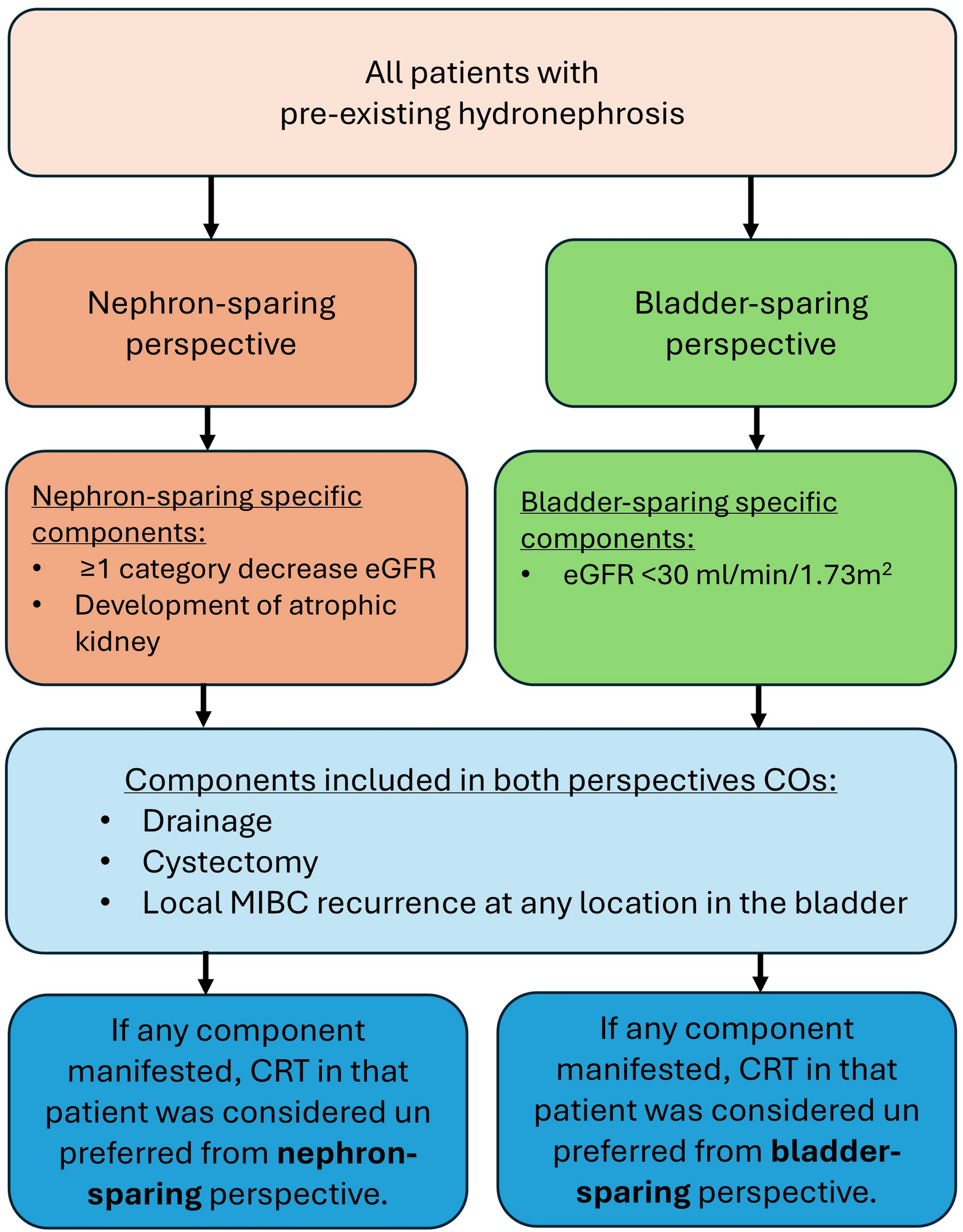
Our findings do not provide a definitive conclusion regarding treatment recommendations. The impact of CRT in the presence of hydronephrosis on long-term eGFR appears mild, although most dilated kidneys probably decrease function. Together with the limited number of cystectomies (2/27) and long-term nephrostomies (9/27) in this group, this suggests that hydronephrosis is a relative rather than an absolute contra-indication for CRT. In our opinion, these findings may support a less conservative view of hydronephrosis as an exclusion criterion for CRT in all patients with MIBC and pre-existing hydronephrosis. These findings showed that hydronephrosis in patients with MIBC persists following CRT and that in 5 out of 9 patients with persisting hydronephrosis who do not undergo drainage, loss of kidney function and/or an atrophic kidney develops (see Supplementary Table 1). Therefore, drainage of the hydronephrotic kidney should be recommended to patients if maximal preservation of functioning kidney tissue is expected and clinically warranted. In our opinion, in patients with hydronephrosis CRT could be proposed to elderly patients, patients with relatively short life expectancy, patients with a high morbidity or mortality risk during and following cystectomy and those who wish to maintain their bladder after appropriate counselling. In Fig. 5 we present a flowchart outlining the ideal management strategy for patients with pre-existing hydronephrosis who prefer bladder-sparing treatment, according to our opinion. However, counselling on potential consequences, such as the need for drainage or, if drainage is refused, the loss of kidney function, remains important. Notably, the high risk of a permanent nephrostomy tube or double-J stent in patients who receive drainage should be addressed during the counselling process. Overall, we recommend that nephron-sparing versus bladder-sparing should be part of patient counselling, and the CO results can help herein.
Fig. 5
Management strategy proposal for patients with pre-existing hydronephrosis. CRT = chemoradiotherapy; DMSA = dimercaptosuccinic acid; MIBC = muscle-invasive bladder cancer
Patients should be counselled on both bladder-sparing and nephron-sparing treatment approaches. In cases where the patient expresses a preference for chemoradiotherapy (CRT) and meets the necessary criteria, a dimercaptosuccinic acid (DMSA) scan should be conducted to evaluate the relative function of the hydronephrotic kidney. In cases where the relative function is less than 10%, CRT can be performed without the need for drainage. However, it is imperative to discuss the risks of complications, such as infection, with the patient. In instances where the relative function is 10% or greater, drainage should be recommended and discussed with the patient. The patient may also opt for cystectomy instead of CRT, if deemed eligible, after the results of the DMSA scan indicate the need for drainage. In cases where drainage is necessary, a percutaneous nephrostomy tube is the preferred procedure, as it minimizes the risk of tumour spread within the urinary tract. In accordance with CRT, the management of the nephrostomy tube (permanent placement, removal, or conversion to a double-J stent) is contingent upon the persistence of hydronephrosis and the residual kidney function.
This study has several limitations. First, its retrospective design, resulting in missing follow-up data, treatment variability and the presence of competing risks (e.g. death), may have influenced hydronephrosis-related outcomes. Second, the presence of hydronephrosis was likely a factor in the treatment decision, resulting in a selection bias. Another limitation is the absence of radiological reassessment of the imaging, to confirm the absence or presence of hydronephrosis.
In conclusion, hydronephrosis in patients with pre-existing hydronephrosis persisted after CRT in 74% (20/27), and 21% (25/119) of the patients without pre-existing hydronephrosis developed hydronephrosis. Drainage was performed in 44% (12/27) of the patients with pre-existing hydronephrosis and in 52% (13/25) of the patients who developed hydronephrosis. Visual complete resection was found to be significantly associated with a decreased risk of development of hydronephrosis in patients without pre-existing hydronephrosis.
Comments (0)