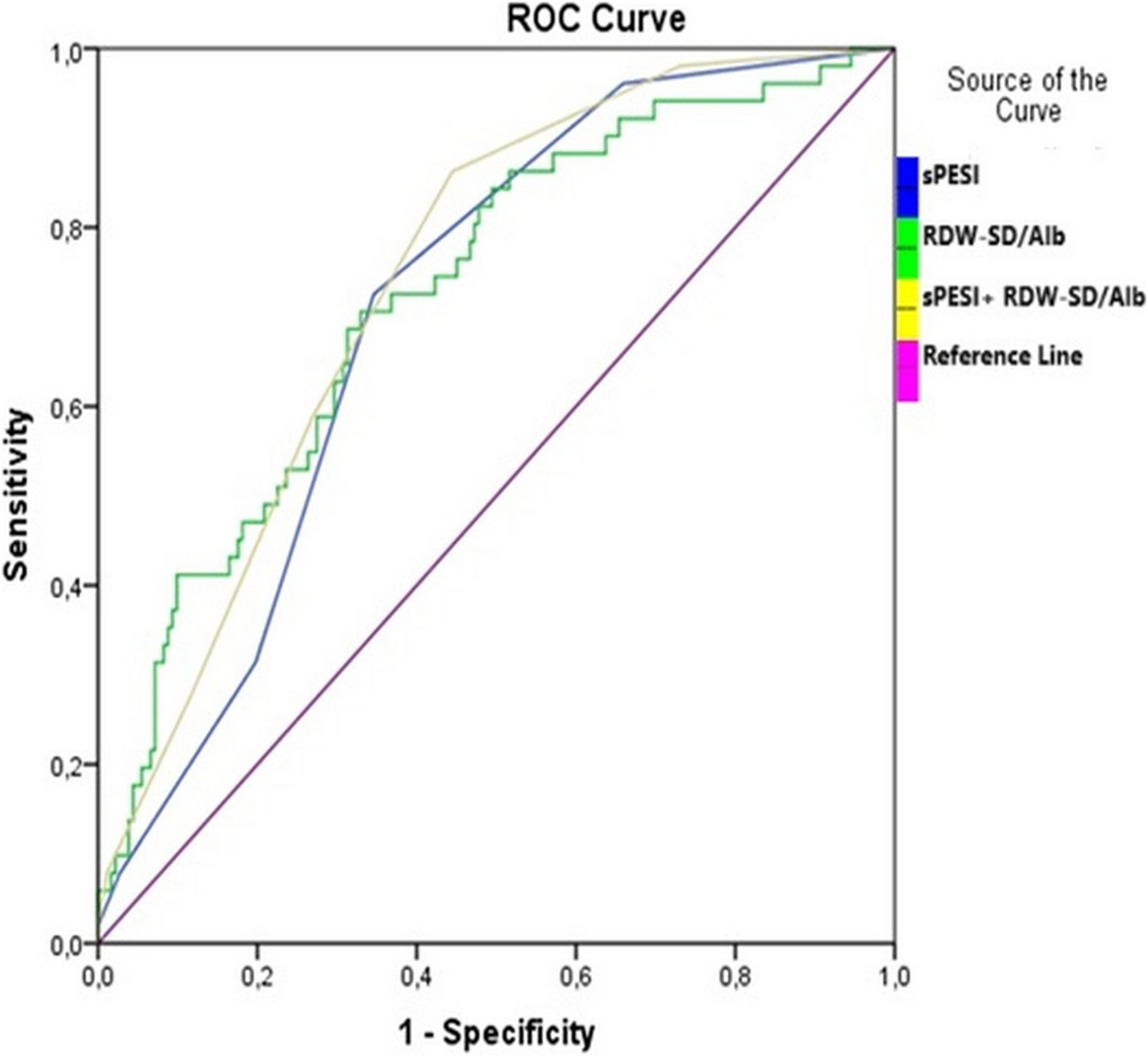
The results of our study identified three main findings: First, the RDW-SD/Alb ratio was higher in the non-survivor group than in the survivor group among patients with APE. Second, the cut-off value RDW-SD/Alb for the predicting 6-month all-cause death was determined to be 13.6. Third, the predictive value of the sPESI score for 6-month all-cause death improved when the RDW-SD/Alb > 13.6 parameter was included. Additionally, each doubling of the RDW-SD/Alb ratio corresponded to a 2.32-fold increase in 6-month mortality. Finally, RDW-SD/Alb level, along with age, diabetes and AST, were independent predictors of 6-month mortality in patients with APE.
The relationship between RDW and venous thromboembolism is complex and is still under investigation. It is well established that various nutritional deficiencies can occur in patients who experience chronic immobilization and declining renal function, both of which are common in individuals with deep vein thrombosis (DVT) and PE. Additionally, hypoxia caused by the obstruction of pulmonary arteries may lead to the hyperactivation of adrenergic and neurohormonal pathways, triggering the release of pro-inflammatory cytokines. Salvano et al. observed that RDW may be elevated due to the intricate interactions among these underlying conditions in patients with APE. [3] Albumin is a medium-sized protein synthesized by the liver and plays a key role in supporting colloid osmotic pressure in the body. Like RDW, albumin is important for the inflammatory response and oxidative stress [10].Numerous studies have indicated that low levels of albumin are related to poor prognosis in patients with APE [6]. In this study, the combination of RDW-SD and albumin, referred to as RDW-SD/Alb, was linked to all-cause mortality in patients with APE, even after adjusting for various other factors.
We found a moderate inverse correlation between RDW-SD and albumin levels (r = −0.353, p < 0.001). This finding suggests a potential link between changes in red blood cell characteristics and the inflammatory or nutritional status of patients with APE. This association may indicate a possible pathophysiological connection and supports the idea that the RDW-SD/Alb could be a useful prognostic marker. However, more research, including larger and more comprehensive studies, is needed to better understand its clinical significance.
APE is classified into three categories based on imaging findings and patient characteristics: high-risk, intermediate-risk, and low-risk. High-risk PE is defined by sustained hypotension, indicated by a SBP of less than 90 mm Hg for at least 15 min or a vasopressor requirement with no other plausible explanation for the shock. Intermediate-risk PE includes patients who exhibit signs of right ventricular (RV) dysfunction through imaging or biomarker evidence (such as myocardial necrosis or chamber dilation) but do not show sustained hypotension. A subcategory of intermediate-risk, intermediate-high-risk PE involves patients with both imaging and biomarker evidence of RV dysfunction. Low-risk PE does not fulfill the criteria for high-risk or intermediate-risk PE [8]. Severe PE patients with SBP greater than 90 mm Hg are categorized according to their risk of hemodynamic collapse and death. Individual risk factor-based clinical prediction scores can be used to identify patient subgroups at high risk for hemodynamic instability. Despite the large number of published clinical prediction scores, only a few numbers have been prospectively validated and shown to be trustworthy [11]. These include the Bova score, the PESI, and sPESI scores. The Bova score combines high troponin levels and RV dysfunction with hemodynamic instability criteria, whereas the PESI and sPESI scores combine markers of cardiopulmonary impairment with age and comorbidities [12, 13]. The European Society of Cardiology guidelines recommend using PESI, an algorithm that calculates various clinical and hemodynamic indicators, to predict 30-day mortality. Due to the complexity of the original PESI, which consists of 11 differently weighted variables, a simplified version called sPESI has been developed and validated. A sPESI score of 0 identifies a low-risk group, with an approximately 1.0% mortality risk within 30 days. In contrast, a sPESI score of 1 or higher identifies a high-risk group, with a 30-day mortality risk increasing to 10.9% [14]. Additionally, markers of RV dysfunction, including ECG, TTE, BNP, and troponin levels, are commonly used for prognostic evaluation in patients with APE. According to retrospective investigations, scoring systems that use biomarkers like the BOVA score are better than the sPESI score at predicting the likelihood of unfavourable events in the early stages [15,16,17,18]. Although the sPESI score is a powerful tool for excluding adverse events in patients with a score of 0, its predictive power for mortality in patients with a score of ≥ 1 is still in doubt. Trimaille et al. examined whether the sPESI score's capacity to predict death was enhanced by including renal dysfunction. [19] The findings demonstrated that a group with extremely high mortality was found when renal failure was included as a biomarker to the sPESI score. This implies that more biomarkers are required to help the sPESI score more accurately predict the likelihood of unfavorable outcomes. The sPESI score was initially developed and validated to predict 30-day mortality in patients with PE. In our study, we did not aim to enhance or recalibrate the predictive ability of the sPESI score. Instead, we utilized it as a baseline tool and included an additional analysis to assess its association with 6-month mortality. Our objective was to investigate whether the sPESI score could provide prognostic insights beyond the originally validated 30-day timeframe. Thus, the study does not change the original purpose of the score but rather examines its extended utility for long-term risk assessment. In the present study, although the sPESI score was higher in the non-survivor group, both groups had high-risk sPESI scores. In light of these findings, RDW-SD/Alb might be thought of as a predictor of all-cause mortality among patients with high-risk features. Furthermore, we observed that the predictive value of the sPESI score for six-month all-cause death improved when RDW-SD/Alb > 13.6 was included as a parameter. Therefore, in addition to the sPESI score, RDW-SD/Alb can be utilized as a biomarker to predict early mortality in individuals with APE more precisely.
Recently, Ding et al. examined the relationship between RAR levels and the risk of all-cause mortality in patients with APE admitted to the intensive care unit (ICU). The researchers categorized the patients into three groups according to their RAR levels: Low RAR (2.68–4.71), Middle RAR (4.71–6.09), and High RAR (6.09–15.45). The study found a significant association between the Middle and High RAR groups and an increased risk of all-cause mortality in patients with PE. [6] Furthermore, our study indicated that higher RDW-SD/Alb (> 13.6) was associated with 6-month all-cause mortality, not only in ICU patients diagnosed with APE but also in all hospitalized patients with this condition.
The RDW-SD/Alb ratio demonstrated significant prognostic value in our cohort; however, the cut-off value of 13.6 was determined through ROC analysis and may not be applicable universally to all populations. Therefore, it should be interpreted with caution and validated in future studies involving independent groups.
Eraslan et al. evaluated the impact of RAR on mortality in patients with PE. [7] Their analysis identified a cut-off value of 5.294 using ROC analysis. Patients with an RAR of 5.294 or higher had a significantly shorter mean survival time compared to those with an RAR below this threshold. In our study, we established that the RDW-SD/Alb cut-off value predicting all-cause death at six months was 13.6. It is important to note that Eraslan et al. calculated the RAR using the RDW-CV (%) unit, whereas we utilized the RDW-SD (fL) unit. We believe the differing cut-off values between the two studies may be attributed to this distinction. Recent studies indicated that RDW-SD may offer additional diagnostic value, as it is a direct measurement that is not influenced by mean corpuscular volume and more accurately reflects variations in red cell size. [20, 21] There is insufficient data in the literature about whether RDW-SD or RDW-CV should be used for calculating RAR.
In this study, we observed a significantly higher 6-month mortality rate among APE patients with elevated RDW-SD/Alb levels. Since hypoalbuminemia is commonly found in cancer patients and malignancy is a well-established risk factor for both mortality and venous thromboembolism (VTE), it may be hypothesized that cancer primarily drives this association [22]. However, the RDW-SD/Alb ratio remained a significant and independent predictor of 6-month mortality, even after adjusting for active cancer in multivariable Cox regression analyses. These findings suggest that the RDW-SD/Alb ratio may act as a reliable prognostic biomarker in patients with APE, regardless of the presence of underlying cancer.
Our study has several limitations. First, it was a single-center, retrospective, observational study, which inherently has limitations due to its design. Second, data on the study population were obtained from our hospital's electronic medical records, which may introduce a selective bias. Third, RDW-SD/Alb is a recently identified inflammatory marker, and a prospective study is necessary to more accurately determine its predictive cut-off value in patients with APE.


Comments (0)