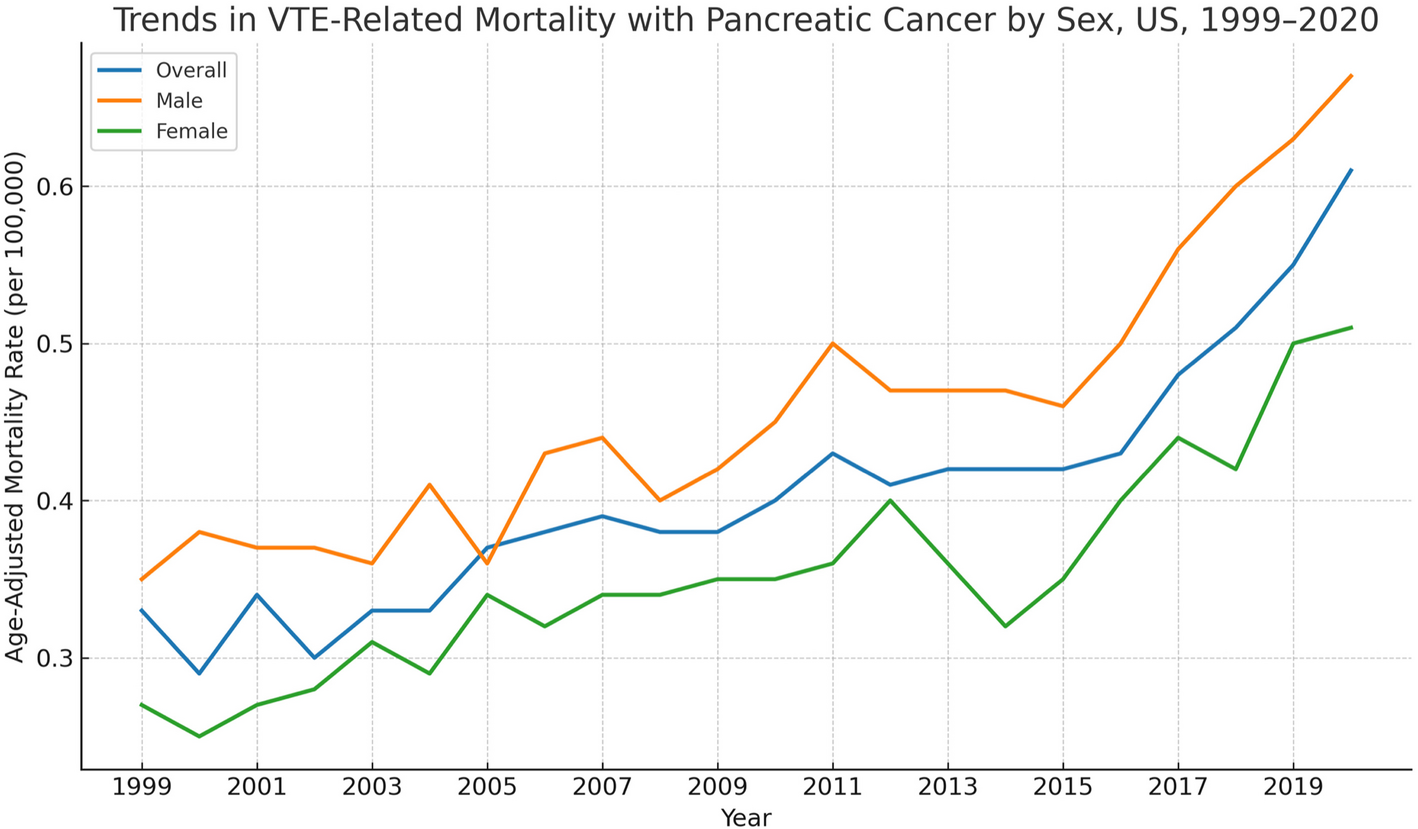
In this nationwide study spanning 1999 to 2020, we identified a clear and sustained rise in venous thromboembolism (VTE)–related mortality among patients with pancreatic cancer in the United States. The overall age-adjusted mortality rate (AAMR) increased steadily throughout the study period, with a particularly sharp rise beginning in 2016. Joinpoint regression revealed three distinct phases, with the most recent segment demonstrating a statistically significant annual percent change (APC) of 8.71%, underscoring the growing burden of VTE in this high-risk population.
The increase in VTE-related mortality was not uniform across all demographic groups. Males exhibited consistently higher AAMRs than females, though both sexes experienced parallel upward trends. Older adults—particularly those aged 75 years and above—had the highest mortality rates, reflecting the accumulation of prothrombotic risk factors with age. We also observed striking racial and ethnic disparities, with Black individuals experiencing the highest mortality burden. Regional and state-level variation further highlighted geographic disparities, suggesting underlying differences in care access, healthcare infrastructure, and resource distribution. Notably, nearly one-third of VTE-related deaths occurred at home, raising important concerns about end-of-life care quality, outpatient VTE recognition, and the role of palliative services. These findings provide a comprehensive national overview of the evolving impact of VTE among pancreatic cancer patients. They underscore the urgency for improved risk stratification, equitable preventive strategies, and targeted interventions to curb this rising mortality trend.
The elevated risk of VTE in pancreatic cancer stems from a complex interplay between tumor biology and host responses. Pancreatic ductal adenocarcinoma (PDAC) is characterized by overexpression of tissue factor (TF) on tumor cells, which directly activates the coagulation cascade and drives thrombin generation [16]. Additionally, PDAC is associated with the release of procoagulant microparticles, systemic inflammation, and neutrophil extracellular trap (NET) formation—all contributing to a hypercoagulable state [17]. These prothrombotic mechanisms are not incidental but rather reflect the aggressive nature of PDAC and may facilitate tumor progression and metastasis via thrombin-mediated pathways [18].
Clinically, VTE is more than a complication; it often marks a turning point in the disease trajectory. Several studies have demonstrated that VTE is an independent predictor of poor survival in pancreatic cancer, associated with both early mortality and treatment interruptions [19]. The onset of VTE may restrict therapeutic options due to bleeding risk or necessitate hospitalization, further diminishing quality of life and survival outcomes. Moreover, VTE can serve as an early indicator of occult malignancy, with pancreatic cancer frequently identified in patients presenting with unprovoked thromboembolism [20].
Despite a well-established understanding of VTE pathophysiology and consequences, underdiagnosis and undertreatment persist in the pancreatic cancer population. While guidelines advocate thromboprophylaxis in high-risk patients, implementation remains inconsistent—often hindered by concerns over bleeding, particularly in those with advanced disease or poor performance status [21]. The increasing VTE-related mortality observed in our study may reflect missed opportunities for early identification, risk-based intervention, and consistent use of prophylactic anticoagulation.
Our findings also reveal substantial disparities in VTE-related mortality across demographic groups. Males consistently exhibited higher AAMRs than females, consistent with broader VTE epidemiology [22]. The underlying mechanisms of sex-based differences remain unclear but may involve hormonal influences, distinct cancer biology, comorbidities, and behavioral factors. Differential access to care, treatment uptake, and physician prescribing practices may further exacerbate these gaps. Age was a dominant factor in VTE-related mortality. Individuals aged 75 years and older exhibited the highest rates, with notable increases in recent years. Age-related hypercoagulability—driven by elevated prothrombotic factor levels, endothelial dysfunction, and decreased mobility—is further intensified in cancer patients by chemotherapy, central venous access devices, and tumor-induced inflammation [23]. Importantly, anticoagulation in older adults is often underutilized due to bleeding concerns, polypharmacy, and frailty, which may contribute to the elevated mortality rates in this group [24]. Racial disparities were particularly striking in our analysis. Black individuals experienced the highest VTE-related mortality rates among all racial and ethnic groups. Prior studies have consistently demonstrated elevated VTE risk and poorer outcomes in Black patients, even after controlling for comorbidities and socioeconomic status [25]. This multifactorial disparity likely reflects a combination of biological predisposition, reduced access to preventive care, diagnostic delays, and lower anticoagulation prescription rates [26]. Structural inequities—including disparities in insurance coverage and systemic healthcare biases—further compound these risks.
We also observed significant geographic variation in VTE-related mortality, with differences across U.S. Census regions and states. The Midwest and West exhibited higher AAMRs than the South, while populous states such as California contributed disproportionately to national VTE-related deaths. These patterns may be attributed to regional differences in healthcare infrastructure, access to specialized oncology and thrombosis care, and uptake of evidence-based thromboprophylaxis practices. Geographic disparities in cancer outcomes are well documented and often linked to differences in provider density, hospital quality, and adherence to clinical guidelines [27]. In the context of VTE, variability in imaging availability, anticoagulation management, and access to multidisciplinary care may contribute to unequal outcomes [28]. Furthermore, many non-metropolitan areas—highlighted in our analysis—may lack timely diagnostic and treatment resources, increasing the risk of missed or delayed VTE management [29]. Socioeconomic factors also play a key role in shaping regional disparities. States with higher proportions of underinsured residents or limited Medicaid expansion often face challenges in cancer care delivery and experience worse health outcomes [30]. Differences in health literacy, cultural attitudes toward medical care, and patient engagement with preventive strategies may also influence regional patterns of VTE diagnosis and treatment.
An often-overlooked dimension of VTE-related mortality in pancreatic cancer is the setting in which death occurs. In our study, nearly one-third of VTE-related deaths took place at home, while the remainder occurred primarily in hospital settings. This distribution raises important considerations about end-of-life care, recognition of thrombotic symptoms outside of clinical environments, and access to timely intervention. The high proportion of home deaths likely reflects a combination of factors. Some patients may have elected home-based palliative care, aligning with care goals that prioritize comfort over aggressive interventions [31]. Others may have succumbed to undiagnosed or untreated VTE events, especially if symptoms such as dyspnea or limb swelling were attributed to advanced cancer and not further investigated. In outpatient and hospice settings, the ability to diagnose and manage acute VTE is often limited due to a lack of imaging capabilities and laboratory support.
Existing literature highlights inconsistencies in the management of VTE during end-of-life care. Treatment decisions are often shaped by provider attitudes, uncertainty about prognosis, and fears of bleeding complications [32]. Although hospice and palliative care teams increasingly recognize the symptomatic burden of VTE—manifesting as painful swelling or respiratory distress—routine anticoagulation remains controversial [33]. A symptom-guided approach, rather than rigid adherence to standard protocols, has been proposed for managing thrombotic complications in this population [34].
The rising trend in VTE-related mortality among pancreatic cancer patients in our study aligns with, yet also expands upon, previous findings from clinical cohorts and population-based registries. Prior studies have primarily focused on VTE incidence rather than VTE-attributable mortality, making this study a unique contribution. For example, a large prospective registry by Frere et al. found that VTE developed in up to 41% of patients with pancreatic cancer during the course of treatment and was independently associated with worse overall survival [2]. However, national-level mortality data reflecting this impact over time have been lacking.
Our finding of a sharp increase in VTE-related deaths after 2016 is consistent with recent reports suggesting that cancer survival improvements may be unintentionally contributing to greater exposure time for thrombotic complications [35]. Longer survival with pancreatic cancer, aided by newer chemotherapy regimens such as FOLFIRINOX and nab-paclitaxel plus gemcitabine, may leave patients vulnerable to cumulative VTE risk. However, these regimens are also associated with high rates of treatment-related complications, including thrombosis [36]. Other studies, such as the Cancer-VTE Registry from Japan, have reported elevated VTE risk in PDAC, but with lower overall incidence compared to Western populations [8]. This may reflect differences in ethnicity, anticoagulation practices, or diagnostic surveillance. Our study, which shows both rising mortality and clear disparities across age, sex, and race, supports the need for contextualized, population-specific strategies in VTE prevention and management.
Furthermore, while many randomized trials have evaluated anticoagulation for VTE prevention in cancer patients—such as the CASSINI and AVERT trials [37, 38]—they have not focused exclusively on pancreatic cancer, nor have they evaluated long-term mortality trends. This reinforces the value of our analysis, which captures real-world outcomes in a particularly high-risk population.


Comments (0)