Primary hyperoxalurias (PHs) are ultra-rare autosomal recessive inborn errors (prevalence 1–3 per 1,000,000) of hepatic glyoxylate metabolism, characterized by overproduction and elevated urinary excretion of oxalate [1, 2]. Three genetic forms of PH (PH1, PH2 and PH3) have been described, caused by mutations of the AGXT, GRHPR and HOGA1 genes, respectively [3, 4]. PH1 is the most frequent and severe PH form, accounting for about 80% of genetically characterized patients [2, 5].
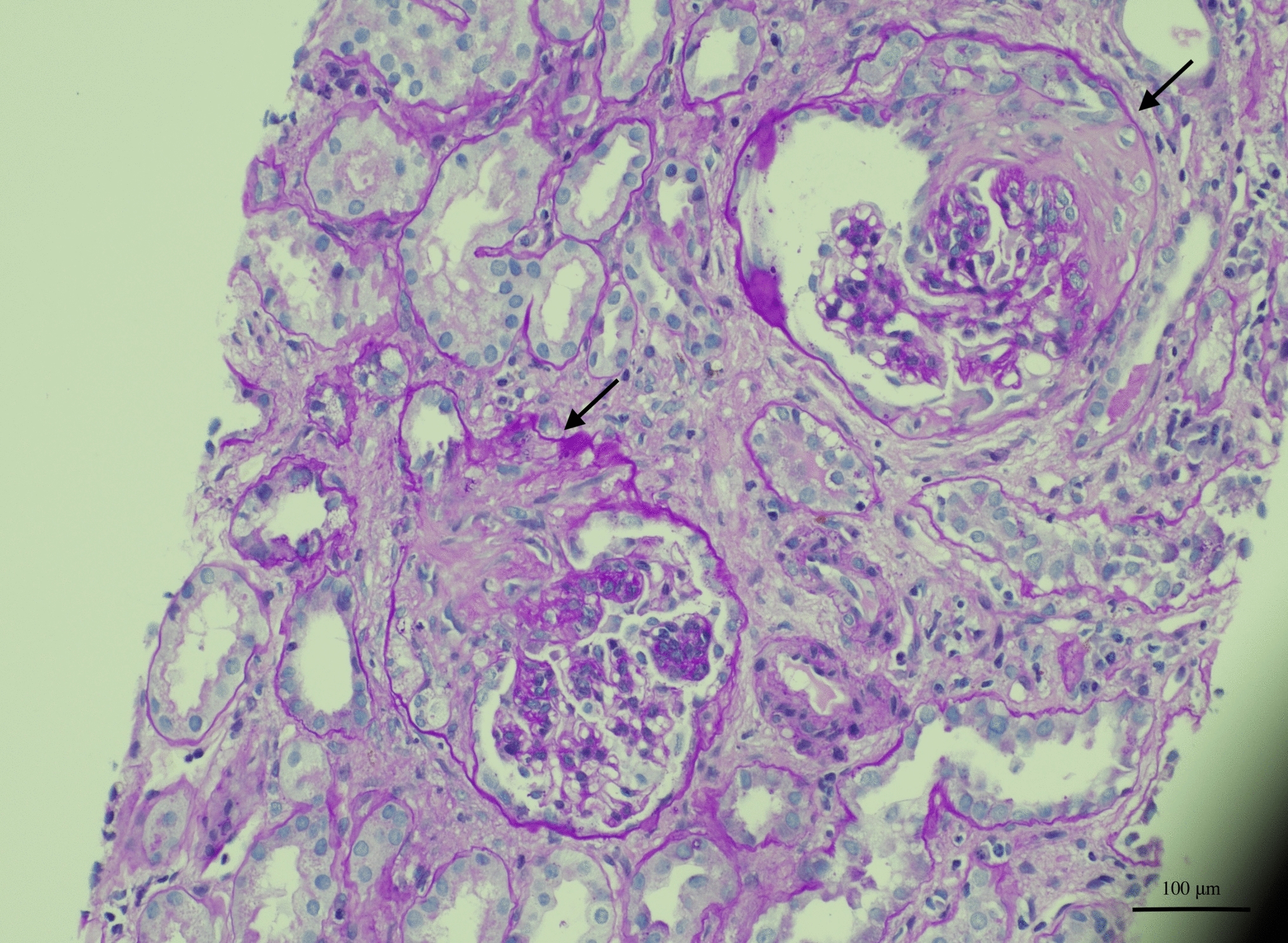
In PH1, the kidneys represent the main target of oxalate crystal accumulation, leading to end-stage kidney disease [6]. As kidney function declines, plasma oxalate levels increase, and systemic oxalosis may develop, causing nephrocalcinosis and kidney failure, as well as osteoskeletal, cardiovascular, ocular, cutaneous, and neurological symptoms [7].
Genetic testing is the gold standard for diagnosing PH, and genetic confirmation and typing of PH are pivotal to managing these patients [8]. Although the onset of PH1 typically occurs in childhood, symptoms can appear later in life and even in adulthood [9, 10]. In adult patients, PH1 presents with phenotypic heterogeneity, ranging from nephrocalcinosis with kidney failure to only occasional stone formation similar to idiopathic stone disease [10]. These factors, along with the rarity of this disorder, are responsible for its underdiagnosis in adult patients, particularly among those undergoing dialysis [4, 11]. In this context, up to 50% of patients have chronic kidney disease (CKD) or kidney failure at diagnosis, and approximately 10% are diagnosed after disease recurrence on kidney allograft [1, 11]. This evidence suggests the fundamental importance of a prompt diagnosis of PH1 to improve patient care and subsequent therapeutic strategies, particularly in the adult setting; it also highlights that the definition and optimal deployment of screening tools for this rare condition represents an unmet need [10].
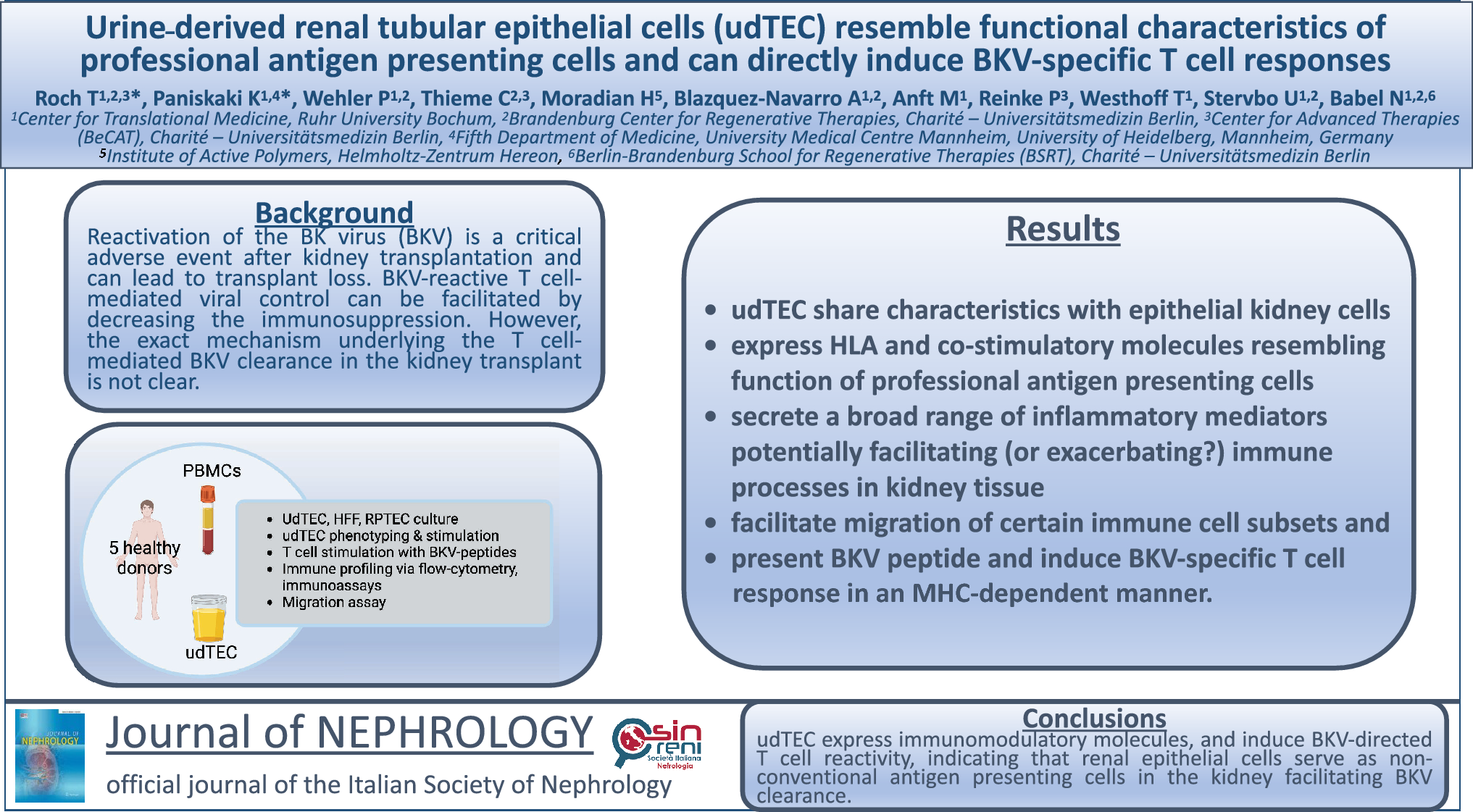
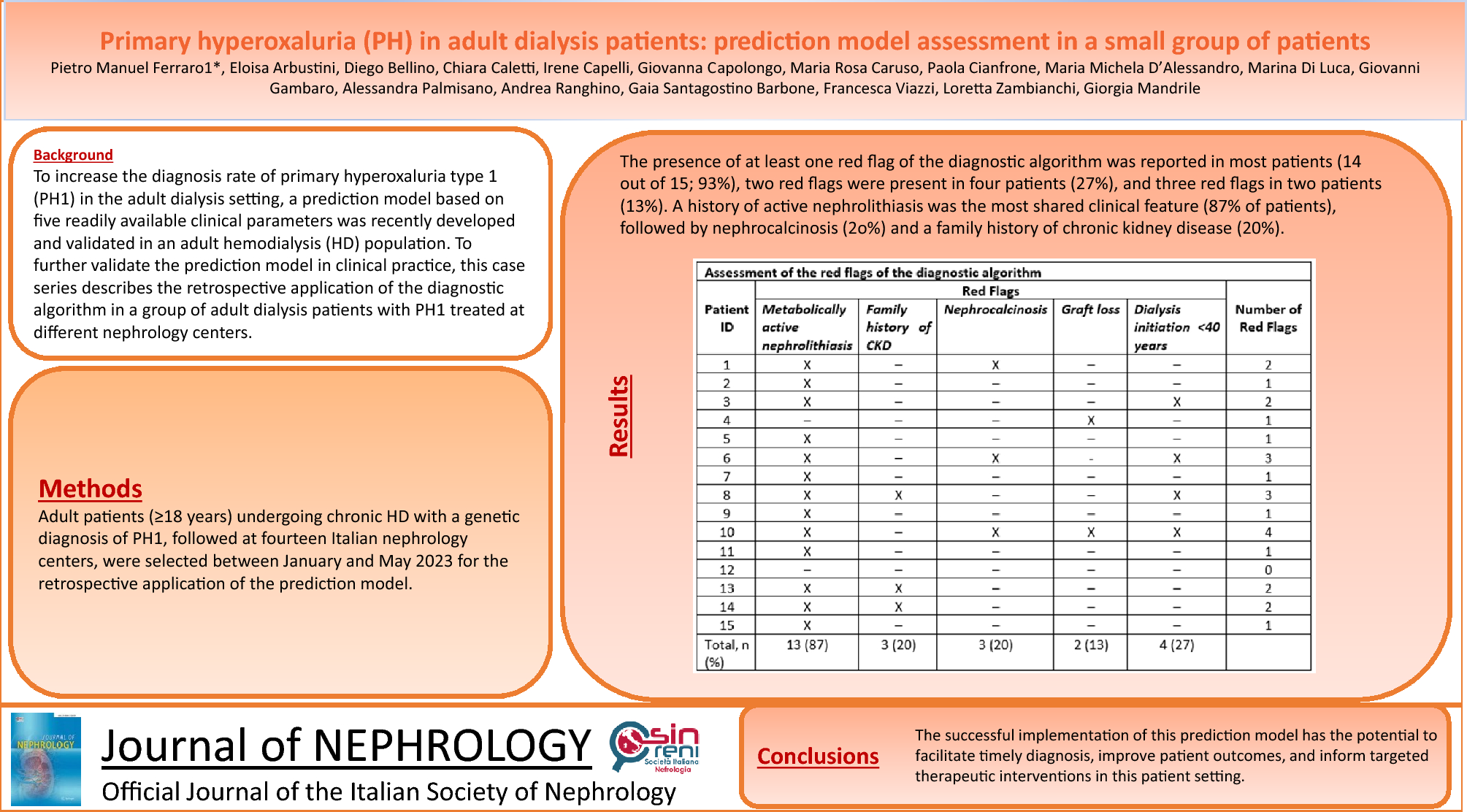
With the aim of increasing the diagnosis rate of PH1 in the adult dialysis setting, we recently developed and validated a prediction model based on readily available clinical parameters in an adult hemodialysis (HD) population [12]. To test our prediction model in clinical practice, we applied to this case series the diagnostic algorithm developed in a group of adult dialysis patients with PH1 treated in several Italian nephrology centers.


Comments (0)