
Remember me

The survey was open for 6 weeks, from May through July 2024, with a total of 100 respondents, of whom 79 self-identified as practicing nephrologists. The 21 respondents that did not self-identify as practicing nephrologists were excluded from analyses.
Fifty-nine (74.7%) participants practiced in the United States with the remaining from 18 other countries. A majority of respondents identified as attending physicians either in an academic center (75.9%) or in private practice (16.5%), and 6.3% were nephrology fellows. Among them, 45.6% identified that they work in a glomerular disease clinic and/or specialize in glomerular disease. Additional questions related to PLA2R, THSD7A, NELL1, and EXT1/2 were further analyzed. Because only few respondents had managed patients positive for the remaining antigens, these were not analyzed further. The demographic and practice characteristics of the respondents are summarized in Supplemental Table 1.
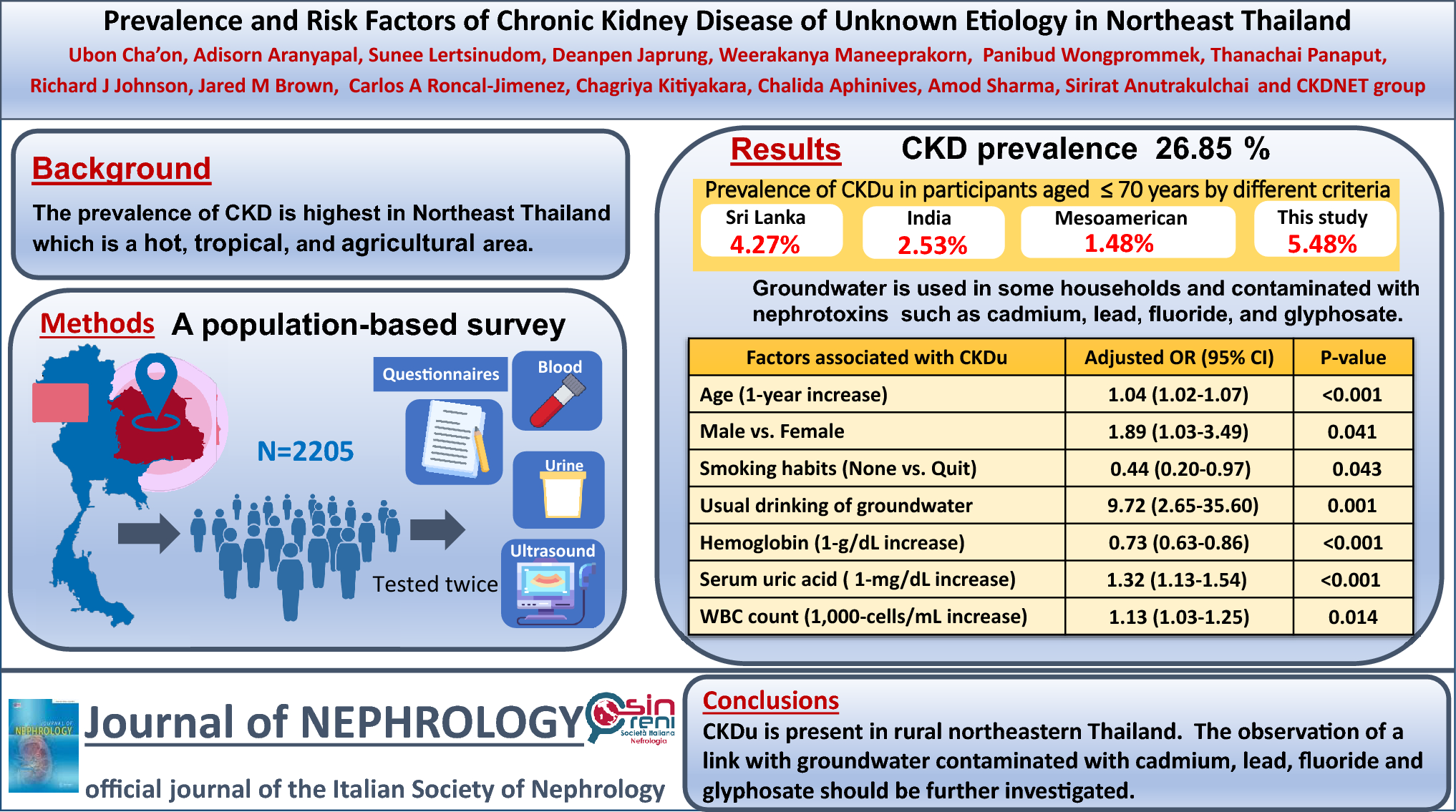
Access to antigen testingIn all countries, respondents reported access to PLA2R testing either performed in-house (45.6%) or by a send-out mechanism (48.1%). For THSD7A, 14.1% of respondents reported having testing available in-house and 43.6% by send-out. This was followed by NELL1, for which 10.1% of respondents reported having testing available in-house and 31.6% by send-out. Finally, for EXT1/2, 6.3% of respondents reported having testing available in-house and 25.3% by send-out. For all other antigens, access to in-house or send-out testing ranged from only 6.4 to 13.9%, and many indicated that access to availability of testing was unknown (Fig. 1, Supplemental Table 2).
Fig. 1
Access to antigen testing. Participants were asked whether the primary pathology lab they send biopsies to performs testing for the antigen in-house or send-out, whether it is not performed, or whether the availability of testing is unknown. A table of values is provided in Supplemental Table 2
Nephrologists were then asked whether they had tested for or treated patients positive for each of the antigens. All respondents had tested for or treated patients positive for PLA2R. Of the other antigens, nephrologists had treated THSD7A (12.7%), NELL1 (15.2%), EXT1/2 (6.3%) positive patients and 1 respondent had treated a contactin-positive patient. Among nephrologists, 46.8%, 21.5% and 17.7% had not treated but had tested for THSD7A, NELL1, and EXT1/2, respectively. Less than 11% of nephrologists had tested for each of the remaining antigens (Fig. 2).
Fig. 2
Testing and treatment of MN patients by antigen status. Participants were asked whether they had tested for and/or treated MN patients positive for each antigen
Evaluation for secondary causes and associationsMembranous nephropathy is associated with various diseases including malignancy, autoimmune diseases, and infections [2]. Included in Fig. 3A–B are the percentages of participants who would screen for these associations for PLA2R, THSD7A, NELL1, and EXT1/2. Supplemental Tables 3–5 are the specific laboratory tests that would be performed for PLA2R-positive MN patients. Similar trends in specific tests performed were obtained for THSD7A, NELL1, and EXT1/2, however, the small number of respondents and questions with multiple answer choices limited these data.
Fig. 3
Screening and treatment practices for patients presenting with MN according to antigen status. A Participants were asked to state how often they screen for malignancy in MN patients by antigen status. B Participants were asked to state how often they screen for non-malignant associated conditions in MN patients by antigen status. C For each antigen, participants were asked what treatment option they would initiate for the MN patient in the prompt. Participants could select multiple answers (n = 69, 8, 10, and 4 for PLA2R, THSD7A, NELL1, and EXT1/2, respectively)
Regarding malignancy workup, a vast majority of participants would perform screening in THSD7A (90%) and NELL1 (81.8%) positive patients (Fig. 3A). For PLA2R-positive patients, the results were dispersed, however 78.6% would screen for malignancy some, most, or all of the time. Notably, for EXT1/2, 20% and 40% said they would never or rarely screen for malignancy, respectively. For the specific tests performed, colonoscopy, mammogram, Prostate Specific Antigen (PSA), PAP smear/HPV testing, and Computed Tomography (CT) scan of the chest were the tests most often performed for PLA2R-positive MN (Supplemental Table 3).
Participants were then surveyed about their workup for non-malignant conditions (Fig. 3B). Notably, 80% would screen for other conditions, including lupus, most of the time in EXT1/2-positive patients. On the other hand, the results for PLA2R, THSD7A, and NELL1 were dispersed across all answer choices. Regarding laboratory tests related to autoimmune and other conditions, for PLA2R-positive MN, ANA, Complement (C3/C4), Serum Protein Electrophoresis, Anti-Double Stranded DNA, and Hemoglobin A1C were most commonly obtained, with other tests having scattered results across respondents (Supplemental Table 4).
Finally, MN has been associated with a variety of infections, particularly HIV, Hepatitis B and C, as well as a few case reports of others such as schistosomiasis [11] or filariasis [12]. We assessed whether physicians screen broadly for multiple infections or focus on ones most associated with MN. As shown in Supplemental Table 5, the most commonly screened for infections in PLA2R-positive MN, were Hepatitis B and C, HIV, followed by syphilis, with others tested for by less than 5% of respondents. Of note, 20.3% said they do not routinely test for infections.
Membranous nephropathy treatment practicesIn this survey, each nephrologist was asked to indicate their preferred initial treatment regimen for a patient with MN positive for PLA2R, THSD7A, NELL1, or EXT1/2. Participants could also choose to continue conservative management. Specifically, participants were asked the following, regarding an MN patient with no contraindications to any immunosuppressive medications:
“The patient has normal renal function and 5g/day of proteinuria, despite maximum tolerated doses of an ACE inhibitor for 3 months. The pathologist informs you that his kidney biopsy was positive for __. What initial regimen would you choose?”
For PLA2R, THSD7A, and NELL1, a large majority chose rituximab (75.4, 87.5, and 80.0%, respectively) (Fig. 3C), while 14.5, 12.5, and 10%, respectively, chose to continue conservative management in this moderate risk clinical scenario.
On the other hand, for EXT1/2, mycophenolate mofetil was chosen by most respondents (75%), although responses were limited. Those that selected mycophenolate mofetil also stated that the antigen affected their treatment decision.
For nephrologists who had treated MN patients with co-existing malignancy, all respondents would ‘Treat the malignancy first and monitor the renal response’ in the setting of THSD7A- and NELL1-positive MN. For PLA2R-positive MN, 67.4% would treat the malignancy first, while 32.6% would treat simultaneously with immunosuppressive therapy specific for PLA2R MN. None of the participants would treat the MN first regardless of antigen status.
Management of M-type phospholipase A2 receptor (PLA2R) membranous nephropathyIn this survey, in addition to the questions for all antigens, participants were asked additional PLA2R-specific questions.
Participants were first asked to state when they would check serum anti-PLA2R antibody levels as a diagnostic test (Fig. 4A). A majority of respondents (82.6%) would perform serum anti-PLA2R antibody testing when nephrotic syndrome is present or when the patient has > 3.5 g proteinuria (spot or 24-h urine) without nephrotic syndrome (68.1%). Overall 33.3% would order the serum anti-PLA2R antibody test when there is > 1 g proteinuria per day (spot test or 24 h urine), and 8.7% would check only after a kidney biopsy has confirmed PLA2R-positive MN.
Fig. 4
Serum anti-PLA2R antibody testing utilization. A Diagnostic value of the serum anti-PLA2R antibody test: Participants were surveyed for their use of the ELISA/IF serum anti-PLA2R antibody test as a diagnostic test. Participants could select multiple answers. Values above each bar correspond to the respective percentage. B Omission of the kidney biopsy: Participants were asked whether and how often they omit obtaining a kidney biopsy in patients with a positive serum anti-PLA2R antibody test. C Use of serum anti-PLA2R antibody test in remission and prognosis: Participants were surveyed for their use of ELISA/IF serum anti-PLA2R antibody levels in their remission criteria. Participants could select multiple answers. Values above each bar correspond to percentages
Participants were then surveyed to determine whether a positive serum anti-PLA2R antibody test would affect their decision to obtain a kidney biopsy (Fig. 4B). Regarding a patient with definitive anti-PLA2R-positive serum testing (ELISA and IF), a majority of respondents (66.7%) reported that they routinely or occasionally omit the kidney biopsy (7.3% and 59.4%, respectively). However, 27.5% would rarely omit the biopsy regardless of serum testing.
Finally, participants were asked if and whether they use serum anti-PLA2R antibody levels to determine remission of PLA2R-positive MN (Fig. 4C). Answer choices could be based on a percent decline from the patient’s baseline and/or by the absolute value. Notably, there was a large spread across all answer choices with a small percentage (10.3%) stating that they do not use immunologic response as part of the remission criteria.
Comments (0)