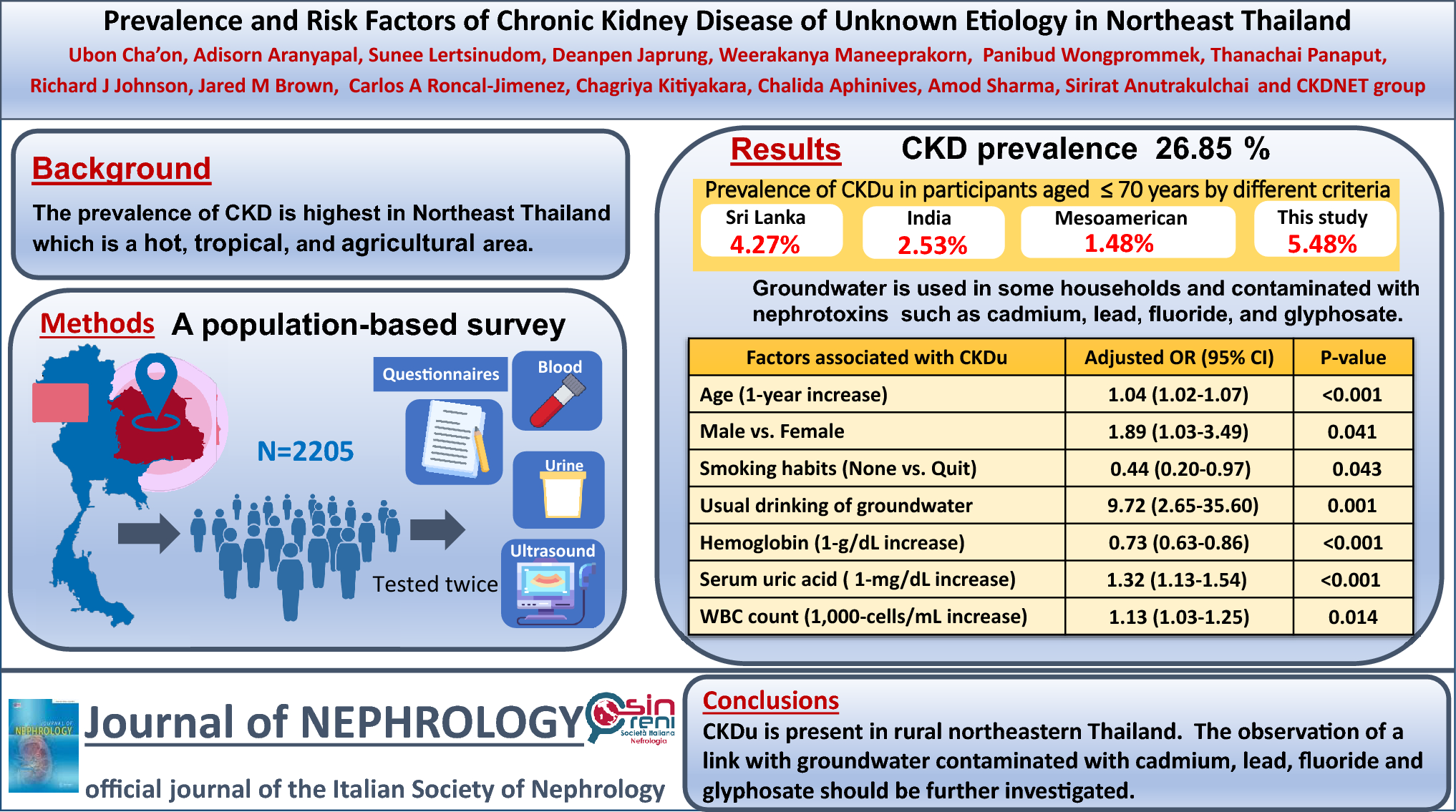
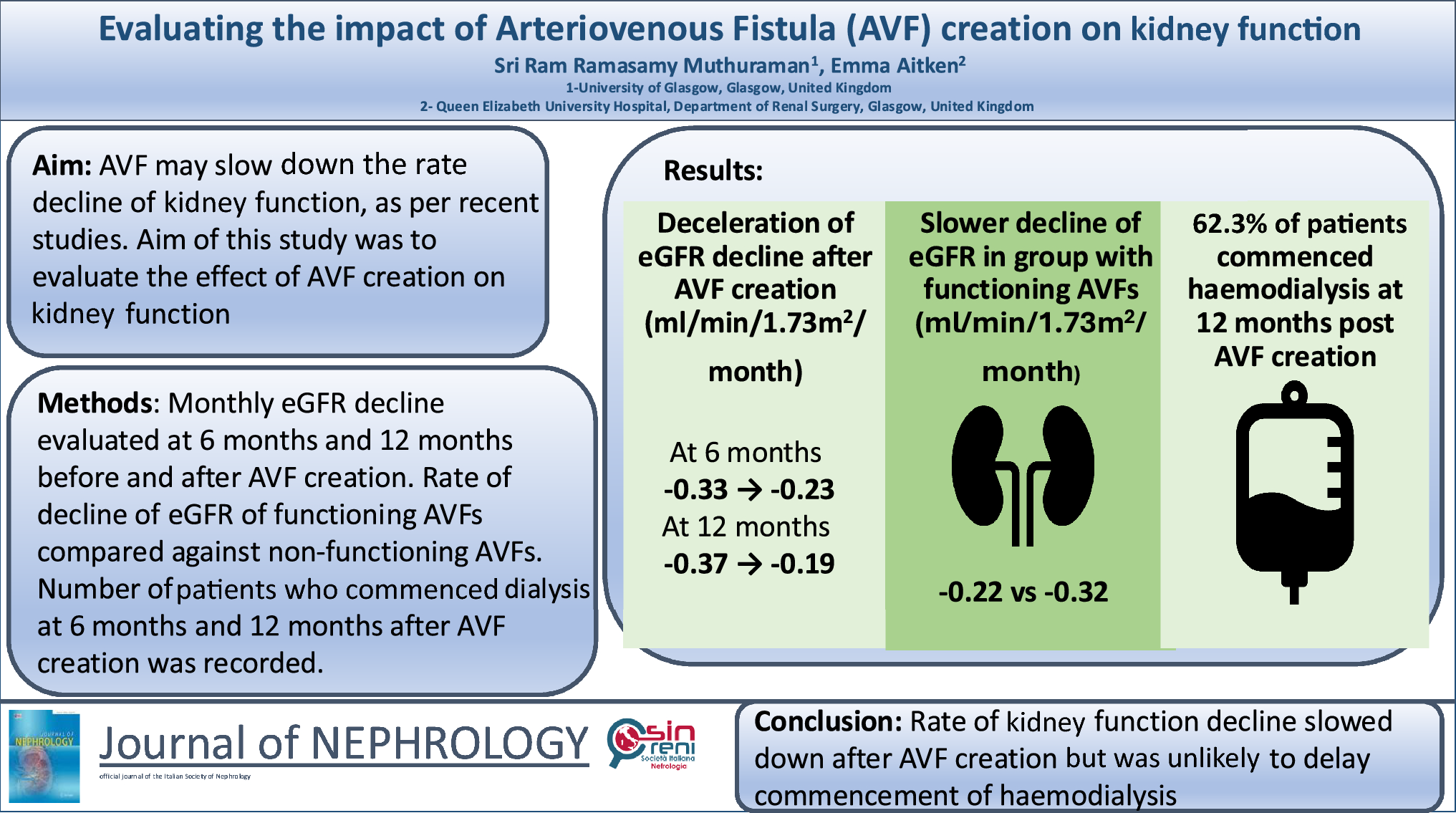
In this single-centre retrospective cohort study, we found that the creation of AVFs reduced the rate of decline in kidney function. When patients with functioning AVFs were compared to those with non-functioning AVFs, the group with functioning AVFs experienced a slower rate of decline after AVF creation. We also found that most predialysis patients commenced haemodialysis in the 12 months post-AVF creation despite the slower rate of decline and the slower increase in their 5-year KFRE score.
The improvement in the rate of decline in patients with kidney failure after the creation of AVFs that we observed was in line with the findings of multiple retrospective cohort studies. Initial studies by Golper et al. on this subject demonstrated improvements in rate of decline after AVF creation [15]. However, this study did not have a control group and used the less reliable 4-variable Modification of Diet in Renal Disease (MDRD) equation that included race as one of the variables when calculating eGFR [17]. Subsequent studies on the impact of AVF creation on kidney function by Dupuis et al. and Sumida et al. reported similar results [12, 14]. These studies involved predialysis patients who were undergoing peritoneal dialysis and predialysis patients who did not have AVFs as control groups, respectively. However, the patients on peritoneal dialysis had fewer co-morbidities and a lower median body mass index (BMI) than patients who had an AVF created [12], and the predialysis patients who did not have AVFs created had a higher prevalence of cardiovascular disease, liver disease and malignancy [14]. Hence, the control groups in these studies were less appropriate. Our study overcame this by having patients who had undergone AVF creation which had then failed to function as our control group. Since these patients were deemed suitable for AVF creation surgery after a pre-operative assessment that accounted for their co-morbidities [18], we can conclude that there was a similar level of baseline health in both the control and intervention groups of our study.
These studies only recorded the rate of decline after AVF creation, which might have limited application to clinical practice. Our study found that while AVF creation may improve the rate of decline and cause a slowing down in the 5-year KFRE in predialysis patients, most of these patients commence haemodialysis in the 12-month period following AVF creation. As such, while AVF creation in the predialysis patient population may delay the initiation of haemodialysis, this is unlikely to be by more than a year post-operatively, thus planning and allocation of resources for the initiation of haemodialysis should still be considered for these patients.
The deceleration of rate of decline following the creation of AVF could be due to the change in renal perfusion and haemodynamics [19]. The arteriovenous fistula creates a relatively low-resistance pathway for blood and this could result in a reduced cardiac afterload [20]. Moreover, as blood flows at a faster rate from arteries directly into the venous system via an AVF, blood is returned to the right atrium and ventricle at a faster rate, resulting in increased cardiac preload. This results in increased left ventricular ejection fraction and increased cardiac output [20,21,22] causing more oxygenated blood to perfuse the kidneys upon the creation of an AVF. As eGFR is inversely proportional to serum creatinine, which is now being cleared at a faster rate through the kidneys due to the increased renal blood flow, the creation of an AVF is associated with a deceleration in the rate of increase of serum creatinine values due to underlying CKD and hence results in a deceleration in the rate of decline in predialysis patients with CKD [12,13,14,15].
Another possible explanation for the deceleration of the rate of decline could be due to remote ischaemic preconditioning [12,13,14,15]. During the creation of an AVF, there is a subclinical steal phenomenon, resulting in relative ischaemia to a distal portion of a limb [12,13,14,15, 23, 24]. This ischaemia can result in a neurohormonal and systemic response which suppresses inflammation and apoptosis [24, 25]. Damage-associated molecular patterns (DAMPs) are released as part of this systemic response, some of which interact with renal tubular epithelial cells to reduce their turnover [24, 25]. DAMPs can also pre-condition the renal epithelial cell to dampen any cellular response to subsequent inflammatory or ischaemic events, which are often the underlying cause of the CKD [24, 25]. This results in the preservation of kidney function, as the renal epithelial cells are less likely to atrophy due to the underlying cause of CKD [26].
Most of the patients in our study commenced haemodialysis within the 12 months following their AVF creation surgery. This is indicative of a progression of their CKD and is likely because predialysis patients for whom AVF creation is indicated already have a lower baseline kidney function [6]. Following AVF creation, kidney function continues to decline, albeit at a slower rate, as the underlying cause of CKD is not treated by the creation of AVF. Hence, while the creation of AVFs may delay the initiation of dialysis in predialysis patients, it is unlikely to prevent this altogether for most patients.
Our study was limited to a single centre and therefore, the results of our study may have limited applicability. However, multiple studies from different centres have reported similar results to our study, which suggests that the findings of our study may be applicable to the wider predialysis patient population worldwide. Our study also relied on observational data and hence, could only identify a correlation between the creation of AVF and the deceleration of rate of decline.
In conclusion, our study found that patients experienced a slower decline in their eGFR and slower increase in their KFRE after AVF creation at both 6 and 12 months. We identified that most patients who undergo AVF creation commence haemodialysis in the 12 months after AVF creation. We also found that patients with functioning AVFs experienced a slower decline in their eGFR compared to patients with non-functioning AVFs at both 6 and 12 months. However, multivariate analysis at 6 months showed that the functional status of AVF was not a predictor of the rate of decline of eGFR. Our study was limited to observational data and hence, a further prospective study should be conducted to ascertain the clinical impact of AVF creation on kidney function and haemodialysis initiation.


Comments (0)