
Remember me
Research among patients in mental health treatment has shown a consistent, positive association between the quality of the therapeutic alliance and treatment outcome across types of treatment and alliance perspectives (e.g., patient or therapist) in both adult [1, 2] and youth studies [3,4,5]. The most recent and comprehensive multi-level meta-analysis of alliance-outcome associations in child and adolescent psychotherapy reported a mean effect size of r = 0.17 (p < 0.001, 62 studies) [5] which was smaller than the effect size in the largest meta-analysis on adult psychotherapy by Flückiger et al. [1] (r = 0.28, p < 0.0001, 295 studies). One explanation for the smaller alliance-outcome associations in child and adolescent therapy may stem from different conceptualizations of the therapeutic alliance between youth and adults [5]. Due to developmental and contextual differences, youth may prioritize different aspects of the alliance compared with adults, and building a constructive therapeutic alliance with adolescent clients may require a somewhat different approach [6, 7].
In youth, studies that included both the alliance perspective of the youth and the therapist demonstrated generally moderate to low [8,9,10,11,12,13,14,15] or nonsignificant agreement [12,13,14,15,16,17] between these two perspectives. Most previous studies that investigated the therapeutic alliance from more than one perspective were in search of the “best” perspective - i.e., which perspective showed the strongest association with treatment outcome. However, there appears to be no “best” perspective: both perspectives on the alliance appear to be predictive of outcome, with effect sizes depending on study characteristics and methodological approach [3, 5].
Perhaps more importantly, the focus on just one perspective tends to ignore the dyadic nature of the therapeutic relationship. The relationship between client and therapist in co-creating the alliance is emphasized in Bordin’s [18] conceptualization of the therapeutic alliance as a partnership. Accordingly, alliance ratings do not refer to a single person or a single perspective but rather to the interaction between the two persons in their relationship [19, 20]. Hence, evaluations of the therapeutic alliance and its association with treatment outcome need to reflect both the client-therapist relationship as well as the client and therapist as individuals.
The social relations model (SRM) [21] provides a conceptual and statistical approach for understanding and analyzing perceptions and actions that occur between pairs of individuals, which can also be applied to the assessment of therapeutic alliance in client-therapist dyads. A modification of the SRM– the ‘one-with-many’ (OWM) model [22]– follows the nested structure which is common in virtually all individual psychological treatments, in which each therapist (‘one’) treats multiple clients (‘many’), but each client is not treated by multiple therapists. Concerning therapeutic alliance in a reciprocal OWM model, in which both the client and therapist rate the alliance, this implies that multiple clients rate the alliance with their therapist, but each client is only rated by one therapist.
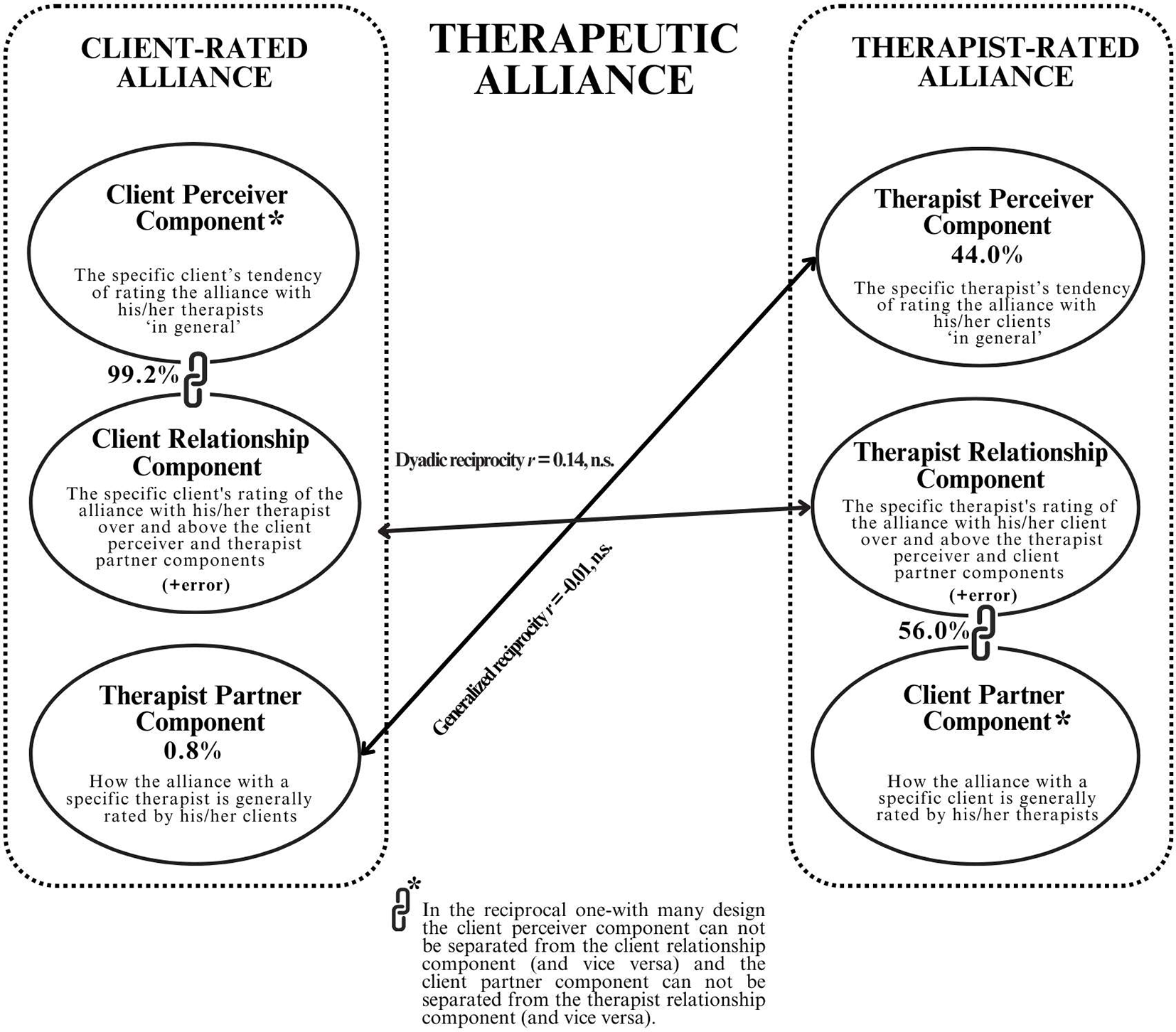
Fig. 1
The Variance Components of the Client- and Therapist-Rated Therapeutic Alliance in the Social Relations Model
Components of variance in the one-with-many model.
When considering the therapeutic alliance in a reciprocal OWM design, three client-related and three therapist-related alliance components are involved (please see Fig. 1). Regarding the client-rated alliance depicted at the left side of Fig. 1, if a client reports a strong alliance with his/her therapist, this in part includes (1) the specific client’s tendency to rate the alliance with therapists ‘in general’ as strong, i.e., regardless of who his/her actual therapist was (the client perceiver component), (2) the specific therapist’s traits and characteristics which elicit a consistent strong alliance rating in most of his/her clients (the therapist partner component), and (3) the specific client’s unique relationship with his/her specific therapist, in which the client rates the alliance as stronger than he/she would have with most other therapists, and stronger than the ratings given by most of the therapist’s other clients, i.e., over and above the client perceiver and therapist partner components (the client relationship component).
Similarly, concerning the therapist-rated alliance depicted at the right side of Fig. 1, if a therapist reports a strong alliance with his/her client, this in part contains (4) the specific therapist’s tendency to rate the alliance with clients ‘in general’ as strong, regardless of who his/her actual client was (the therapist perceiver component), (5) the specific client’s traits and characteristics which elicit a consistent high alliance rating in most therapists (the client partner component), and (6) the specific therapist’s unique relationship with his/her specific client, in which the therapist rates the alliance with the client as stronger than for his/her typical client, and stronger than the ratings most other therapists would have given had they been treating this client, i.e., over and above the therapist perceiver and client partner components (the therapist relationship component).
The reciprocal OWM design presents two major advantages over commonly employed analytical approaches in alliance research. First, the OWM design takes the interdependence in alliance data into account by distinguishing different alliance components. Second, the interdependence in the data can be used to estimate generalized reciprocity– are therapists who report strong alliances with their clients also perceived to form strong alliances by their clients (i.e., the correlation between the therapist-receiver and therapist partner component; see Fig. 1), and dyadic reciprocity– if a client reports a unique strong alliance with the therapist, does the therapist also report a unique strong alliance with that client (the correlation between the client relationship and therapist relationship component). However, compared with the SRM ‘round-robin’ structure in which each individual rates and is rated by every other individual, the reciprocal OWM-design has a limitation in differentiating all alliance components. Because in the reciprocal OWM design each client provides alliance data pertaining to his or her therapist only, and not multiple therapists, the client perceiver component cannot be separated from the client relationship component (and vice versa), because we do not know whether the client would have provided different alliance ratings had he/she been treated by a different therapist. Moreover, because only one therapist provides alliance data regarding one client, the client partner component cannot be differentiated from the therapist relationship component (and vice versa), because we do not know if different therapists who had treated the same client would have provided similar alliance ratings. Therefore, in the reciprocal OWM design four instead of six sources of variance can be distinguished: the therapist-partner and client relationship (+ client perceiver) components in client-rated alliance and the therapist-perceiver and therapist relationship (+ client partner) components in therapist-rated alliance.
Despite the advantages of the reciprocal OWM design this design is rarely used in alliance studies. Only three studies on therapeutic alliance to date - two among adults [23, 24] and one among youth [25] - have used this design to partition alliance variance components and investigate their association with treatment outcome. These studies showed consistent findings regarding variance partitioning, dyadic reciprocity, and a positive relation between the combined client relationship + client perceiver component and treatment outcome. However, therapist-related associations with treatment outcome showed equivocal results.
The present study is part of the Professional Alliance with Clients in Treatment (PACT) initiative in which we earlier investigated the value of incorporating first-session therapeutic alliance ratings from both clients and therapists for predicting 4-months treatment outcome in a youth mental health and youth addiction treatment setting, which showed that youth with a strong alliance according to both perspectives had an eightfold odds of favorable treatment outcome compared with youth with a weak alliance according to both perspectives. In a second study among these youths, we conducted a controlled trial in which we compared a client feedback intervention as an add-on to treatment as usual (TAU) versus TAU-only, which indicated that the client feedback intervention did not show better 4-months treatment outcomes or better alliances than TAU [26]. In the present study in the same youth sample, we used the reciprocal OWM model to investigate the composition of the therapeutic alliance at the first treatment session, with regard to (1) the amount of variance accounted for by the various therapeutic alliance components– with a specific focus on the therapist perceiver and therapist partner component, (2) the presence or absence of generalyzed and/or dyadic reciprocity, and (3) the association between the client-rated and therapist-rated alliance components with treatment outcome.
Comments (0)