This is the first study to provide valuable insights into ADHD prevalence and associated pregnancy-related risk factors among preschoolers in the urban Chinese context, addressing a notable research gap. Our retrospective cohort study revealed that 3.9% of mothers were diagnosed with maternal thyroid dysfunction and 9.9% of children were at high risk for ADHD. The main findings also validated our hypothesis, demonstrating the effects of maternal thyroid dysfunction and stress during pregnancy significantly increase the risk of offspring ADHD, even after controlling for covariates. Furthermore, the analysis underscores the particularly significant impact of stress during the first trimester on ADHD risk, highlighting the critical need for early psychological screening and care in pregnancy.
This study identified that 9.9% of preschoolers were at high risk for ADHD, closely aligning with the prevalence rates in the US, which range from 10.08 to 10.47% [3], and exceeding the global prevalence of 7.6% [2]. Notably, the prevalence rate of ADHD among Chinese preschoolers from 20 kindergartens in our sample surpasses the 7.5% prevalence observed in school-age children from rural Chinese counties [6], and the 6.5% prevalence from a systematic review of 67 studies involving 642,266 Chinese children and adolescents [5]. One possible explanation for these discrepancies is the younger age of our sample (mean age of 4.74 /years) compared to the older age (mean age of 12.36 years) in Pang et al.‘s study. Additionally, our use of the SNAP-IV [24] as a screening and diagnostic tool may identify more potential cases than Pang et al.‘s study in which children have already received a formal ADHD diagnosis [6].
Maternal thyroid dysfunction during pregnancy was associated with an increased risk of ADHD (HR = 1.541), consistent with the findings from a meta-analysis and a longitudinal study in Taiwan [8, 10]. The meta-analysis identified 29 eligible studies and found a significant association between maternal hypothyroidism and an increased risk of ADHD (OR = 1.14) [8]. Similarly, a longitudinal study in Taiwan reported that prenatal hyperthyroidism significantly increased the risk of ADHD in offspring (OR = 2.23) after adjusting for demographic factors and maternal mental health disorders [10]. These findings support the role of maternal thyroid dysfunction as a potential risk factor for ADHD in offspring. This underscores the importance of maintaining thyroid function for both maternal and children’s health. Ge and colleagues further supported this by indicating that maintaining balanced TSH levels during gestation is essential for fetus neurodevelopment [8]. Two reasons may explain this significant association. Firstly, the thyroid hormones are critical regulators in the early development of the fetal brain, including the differentiation of neurons, oligodendrocytes, astrocytes, and microglia [34]. Furthermore, fluctuations in maternal thyroid hormone levels during pregnancy are associated with an increased risk of spontaneous miscarriage, stillbirth, and low birth weight infants, which may contribute to an increased risk of ADHD [35, 36]. However, treatment for thyroid dysfunction during pregnancy remains a controversial issue [37]. Our findings underscore the necessity of developing optimal preventive and management strategies for maternal thyroid dysfunction (e.g., hyperthyroidism and hypothyroidism) during pregnancy. For instance, levothyroxine treatment is encouraged to be utilized based on the TPOAb status and serum TSH levels [38].
Maternal stress across different pregnancy trimesters was a crucial factor in assessing the risk of ADHD in offspring. High maternal stress in the first trimester of pregnancy was significantly associated with a higher risk of ADHD, which partially aligned with previous studies [14,15,16], but contrasted with one study [39]. Compared to children whose mothers were under significant stress, children born to mothers with moderate and minor stress levels during the first trimester had a 36.3% and 42.9% decrease in ADHD risk, respectively. Some mothers may feel physically stressed as they adapt to early pregnancy reactions such as nausea and vomiting. Additionally, maternal stress can induce the secretion of cortisol and glucocorticoids, triggering inflammatory responses that may disrupt fetal hormone levels and contribute to atypical development [40, 41]. There are two potential explanations for this association. On the one hand, stress during pregnancy can also lead to concurrent depression and anxiety in mothers, which may lead to antidepressant impacts on ADHD risk [14, 42]. On the other hand, mothers with stress and depression may engage in unhealthy lifestyle behaviors, such as smoking and overeating, which can negatively impact prenatal neurobiological influences on ADHD risk [15].
We found no significant association between maternal stress during the second and third trimesters and ADHD risk, which aligns with findings from Andreasen et al. [43] but contrasts another study reporting a strong link [39]. These discrepancies may arise from differences in the assessment of stress (e.g., cortisol vs. Perceived Stress Scale) and ADHD (e.g., The Conners Comprehensive Behaviour Rating Scales vs. SNAP-IV). A possible explanation for the non-significant association involves the timing of fetal brain development and maternal protective mechanisms [44]. After 13 weeks of gestation, the maturing fetal hypothalamic-pituitary-adrenal axis and the placental 11β-hydroxysteroid dehydrogenase type 2 enzyme, which inactivates cortisol, may buffer the adverse effects of maternal stress [45]. Further research is needed to clarify these mechanisms and incorporate objective measures to better understand the link between prenatal mental health and fetal neurodevelopment.
Strengths and limitations
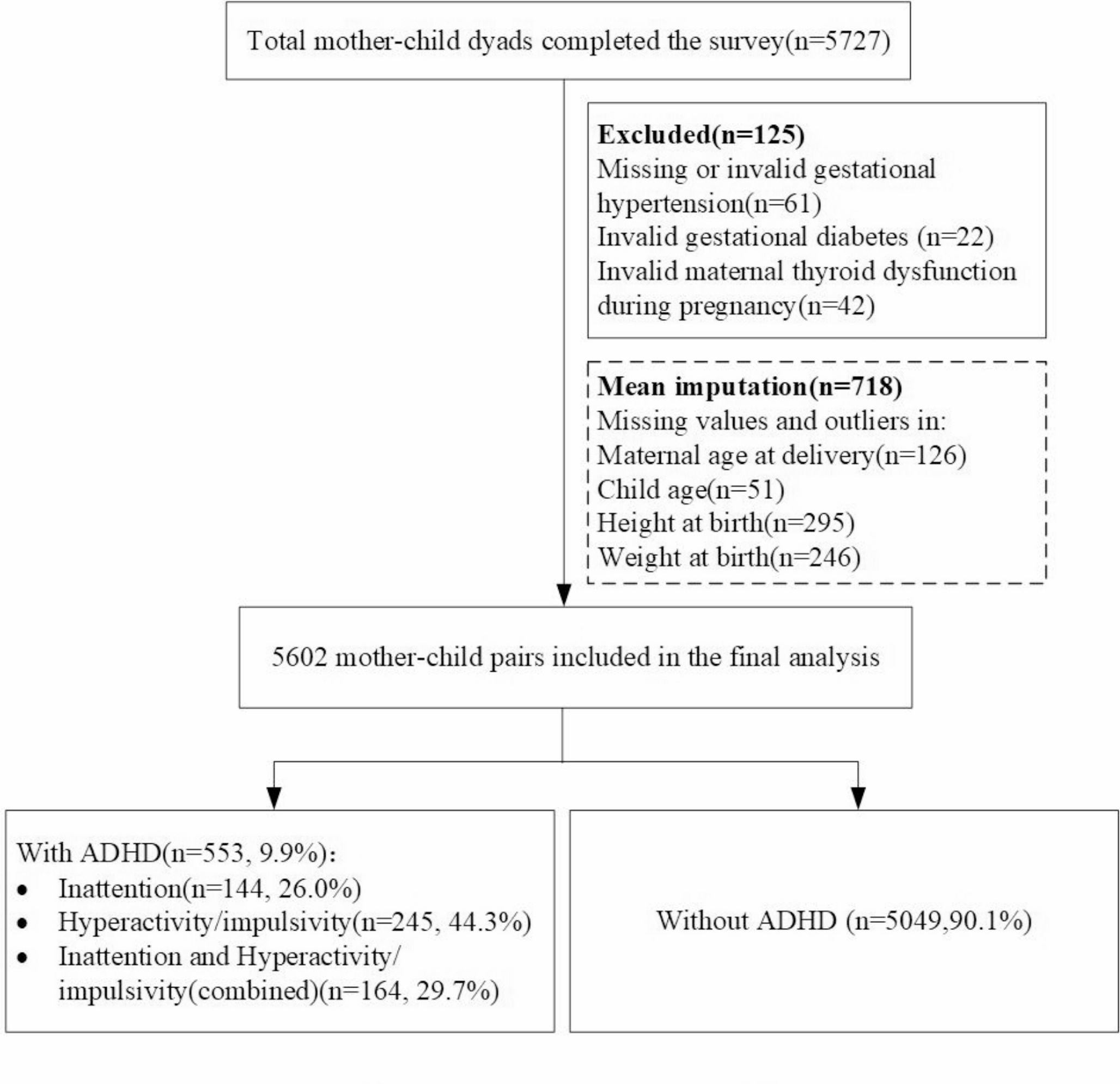
This study has several notable strengths. Guided by the Biopsychosocial Model (George Engel,1977), the study deepens our understanding of ADHD’s etiology by concurrently examining the effects of physiological (thyroid dysfunction) and psychological (stress) factors during pregnancy, with social factors controlled as covariates. Moreover, a pioneering aspect is its identification of potential ADHD cases and associated pregnancy-related factors in a large sample of 5,602 preschoolers from 20 urban Chinese kindergartens. This large-scale, population-based design facilitates the acquisition of a more representative population sample. Additionally, our research contributed to the existing literature by demonstrating that maternal thyroid dysfunction during pregnancy was associated with a 54.1% increase in the risk of ADHD in offspring in urban China. Lastly, while previous studies have examined the link between maternal mental health and offspring ADHD risk, they have not specifically investigated the effects of stress across individual trimesters [14, 15]. Our study filled this gap by being the first to explore the association between maternal stress in different trimesters and the risk of ADHD in offspring. We found that maternal stress during the first trimester of pregnancy was particularly influential. Therefore, implementing preventive approaches to mitigate maternal psychological stress in the first trimester is vital for offspring neurodevelopment.
This study has several limitations. First, all outcome assessments relied on maternal self-reports, which might induce recall or social desirability bias. Future studies are suggested to consider clinician-reported data or laboratory tests (e.g., TSH levels, cortisol levels, and ADHD diagnostic data) obtained from medical records to enhance the objectivity of the findings. Second, our study data was collected from 20 kindergartens in a single region, so the generalizability of findings to other regions might be limited. Third, as the retrospective cohort design may suggest potential causal links between exposure and outcomes, it cannot provide definitive evidence of causality. Hence, well-designed longitudinal studies are warranted to strengthen causal inferences. Fourth, we employed non-validated questions to evaluate maternal stress throughout the pregnancy trimesters, and the omission of a ‘no stress’ category could have led to certain misclassifications. Although these questions provided valuable insights, the absence of a standardized and validated scale may compromise the comparability of our findings. Fifth, the absence of data on maternal antidepressant uses and postnatal psychological outcomes of mothers limited our in-depth understanding of pregnancy factors in the offspring’s ADHD development. Moreover, thyroid dysfunction was recorded only as a binary variable (yes or no); further research should examine its types, duration, and treatment. Future research is suggested to adjust for these potential confounders or biologically relevant covariates to more accurately examine associations.
Implications
Here are some implications for clinicians and policymakers. Firstly, given the 9.9% prevalence rate of high-risk ADHD in offspring aged between 3 and 7 years, promoting early detection in kindergartens or during routine pediatric check-ups can enhance the outcomes for children with ADHD. Furthermore, it is essential to implement effective strategies for treating maternal thyroid dysfunction and maintaining thyroid hormone stability. Moreover, our research underscores the importance of preventing or mitigating maternal stress during pregnancy, particularly in the first trimester. Lastly, targeted ADHD screening for children born to mothers who experienced thyroid dysfunction or significant stress during pregnancy could enhance both detection rates and long-term outcomes in children and mothers. Consistent with the Biopsychosocial Model, our main findings underscore the importance of concurrently considering psychological and physical factors (such as thyroid dysfunction and stress during pregnancy) together. Therefore, it is advisable to offer family-centered screening and treatment programs, considering the family as a holistic unit of care, for preschoolers and mothers who have mental disorders or experienced thyroid dysfunction during pregnancy.

Comments (0)