Study design
This study is part of the SONRIE study, a randomized controlled trial (RCT) registered at ClinicalTrials.gov (Identifier: NCT05849792). It adheres to the 2013 Declaration of Helsinki, approved by the Andalusian Biomedical Research Ethics Portal (1875-N-18 CEI/ Cádiz). All participants provided written informed consent prior to inclusion.
Eligibility criteria included adults aged 25 to 65 years due to the highest prevalence of depression in this demographic in Andalusia [27], with a psychiatric diagnosis of mild-to-moderate depression according to International Classification of Diseases 10th Revision (ICD-10) criteria [28]. We limited our study to individuals with mild-to-moderate depression to ensure participants safety and to maintain a homogeneous sample, as physical exercise has been shown to be an effective intervention in this population [29]. Project investigators subsequently verified that participants met the remaining criteria, including the ability to engage in physical activity without restrictions. Exclusion criteria included a diagnosis of major depression, the presence of acute or terminal illness, a history of cerebral infarction, epilepsy, or brain cancer, and unstable cardiovascular disease or other medical conditions that could interfere with participation in physical exercises.
Participants
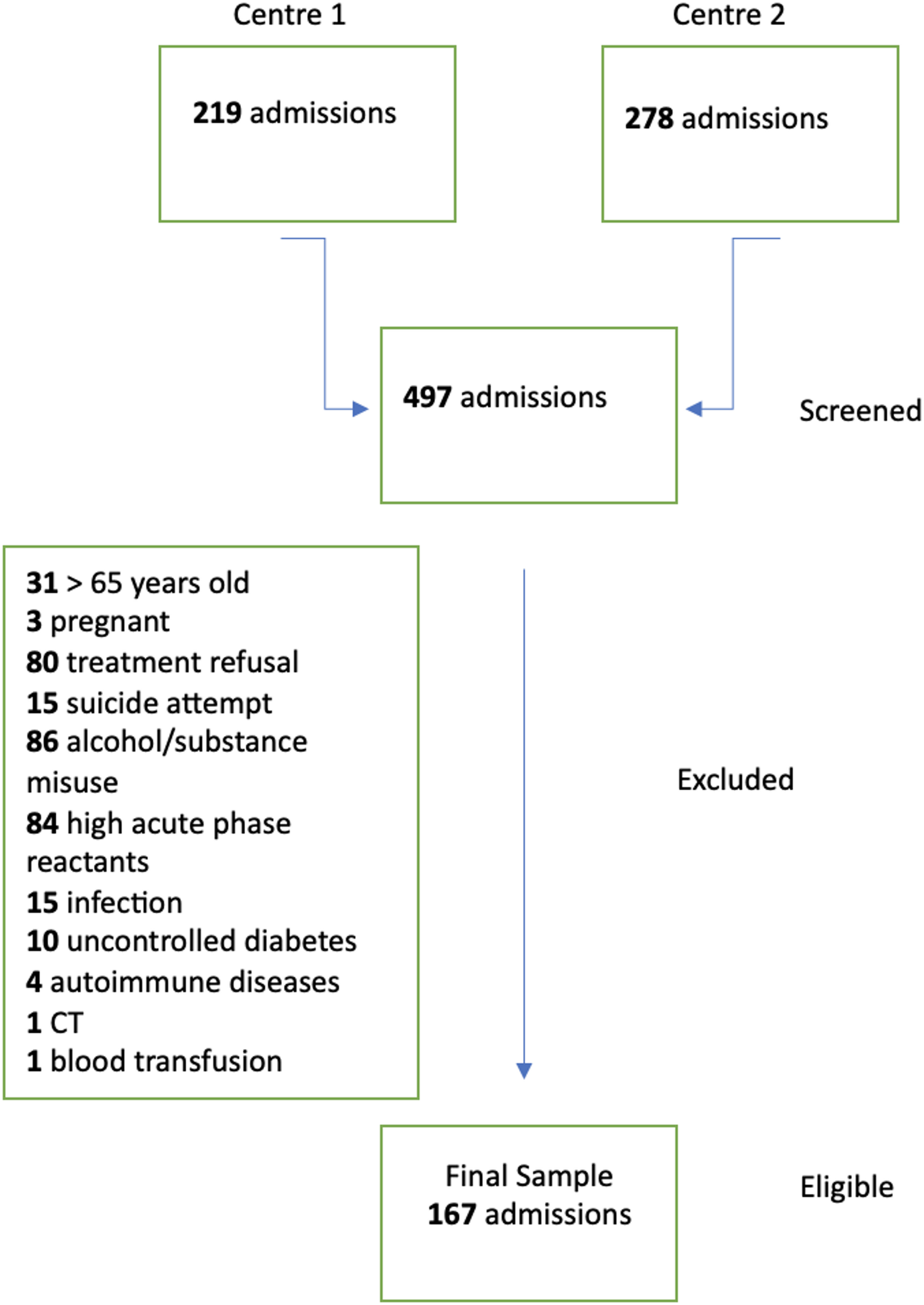
The SONRIE study engaged 132 individuals diagnosed with depression by a psychiatrist from the Mental Health Services of Puerto Real (Cádiz). All participants were in a stable, post-acute phase of depression, and were recruited through a detailed outreach process that included community presentations and social media campaigns. Of these, 120 attended an information meeting and 94 requested the pre-screening questionnaire. After assessing for eligibility, 84 individuals met the pre-screening criteria and 80 were eligible for final assessment.
MeasuresInterview measures
Sociodemographic characteristics were collected using a self-designed developed structured questionnaire. The data captured included age, antidepressant usage, economic stress, smoking and alcohol intake, educational level, and marital status. Additionally, information on comorbidities and the impact of bodily pain on daily functioning was obtained by asking whether participants had ever been diagnosed with conditions such as cardiovascular diseases, cancer, or diabetes (recorded as ‘yes’ or ‘no’). Responses for antidepressant usage and economic stress were binary (“yes” or “no” for medication usage; “easy” or “difficult” for economic stress). Smoking status and alcohol intake were classified into three categories: “current”, “former” or “never”. Educational level was dichotomized into “up to primary education” or “higher education”, and marital status was coded as “single” or “in a relationship”. The persistence of depression was recorded as the number of years since the diagnosis.
Physical appraisalBody composition
Body composition was assessed using a multifrequency bioimpedance analyzer (TANITA-MC780MA) and a stadiometer (Type SECA 225). Specifically, body weight (kg), height (cm), body mass index (BMI, kg/m²), fat mass (kg), fat mass percentage, lean mass (kg), and lean mass percentage variables were measured. Height was measured in the Frankfurt plane, and BMI was calculated using the recorded weight and height values.
Plasma levels of endocannabinoids and endocannabinoids analogues
After an overnight fast, blood sample were collected from each participant between 08:00 and 09:00 h. through venepuncture into K2-EDTA tubes. The plasma was then immediately separated from these samples in a centrifuge pre-cooled to 4ºC, operating at 1700 G for 15 min. This process commenced within 10 min post-extraction to ensure sample integrity. To stabilize the plasma, and prior to freezing, 8 µL of orlistat (250 µg/mL in ethanol) were added to each cryotube designed for ES analyses. After centrifugation, 1 mL of plasma was aliquoted into these cryotubes, which were then stored at -80ºC until analysis. We quantified eCBs (2-AG and AEA) and their analogues (2-LG, 2-OG, OEA, DEA, DHEA, LEA, and SEA) following a previously validated method [30]. Briefly, aliquots of 0.5 mL of plasma were transferred to 12 mL glass tubes, spiked with deuterated internal standards (AEA-d4, DHEA -d4, LEA-d4, OEA-d4, 2-AG-d5, and 2-OG-d5), diluted with 0.1 M ammonium acetate buffer (pH 4.0), and extracted with tert-butyl methyl ether. The dry organic extracts were reconstituted in 100 µL of a mixture water: acetonitrile (10:90, v/v) with 0.1% formic acid (v/v) and transferred to HPLC vials. A Waters Acquity UPLC system with a Xevo TQ-Smicro Mass Spectrometry detector was used for the analysis. Chromatographic separation was performed with a Waters BEH-C18 column (2.1 × 100 mm, 1.8 μm particle size) maintained at 55 °C with a mobile phase flow rate of 0.4 mL/min. The composition of the mobile phase was: A: 0.01% (v/v) formic acid in water and B: 0.01% (v/v) formic acid in acetonitrile. The mass spectrometry analysis was performed on the multiple reaction monitoring mode (MRM). Quantification was performed absolutely by isotope dilution. Quality control samples were injected across four batches, yielding RSDs of 7.0–10.7%. The deuterated internal standards were obtained from Cayman Chemical (Ann Arbor, MI, USA) and Toronto Research Chemicals (Ontario, Canada), and solvents were from Merck (Darmstadt, Germany). Plasma concentrations of 2-AG and AEA were further compared against normative values reported by Hillard et al. [31] to provide additional context.
Health related physical fitness
Cardiorespiratory fitness (CRF) was evaluated using the 6-Minute Walking Test (6MWT). Participants were instructed to walk as fast as possible for six minutes along a flat, 60-meters circuit, aiming to cover the maximum distance possible [32]. The total distance covered in a single trial was recorded in meters for further analyses. Expected 6MWT performance values were calculated using the predictive equations proposed by Enright and Sherrill [33].
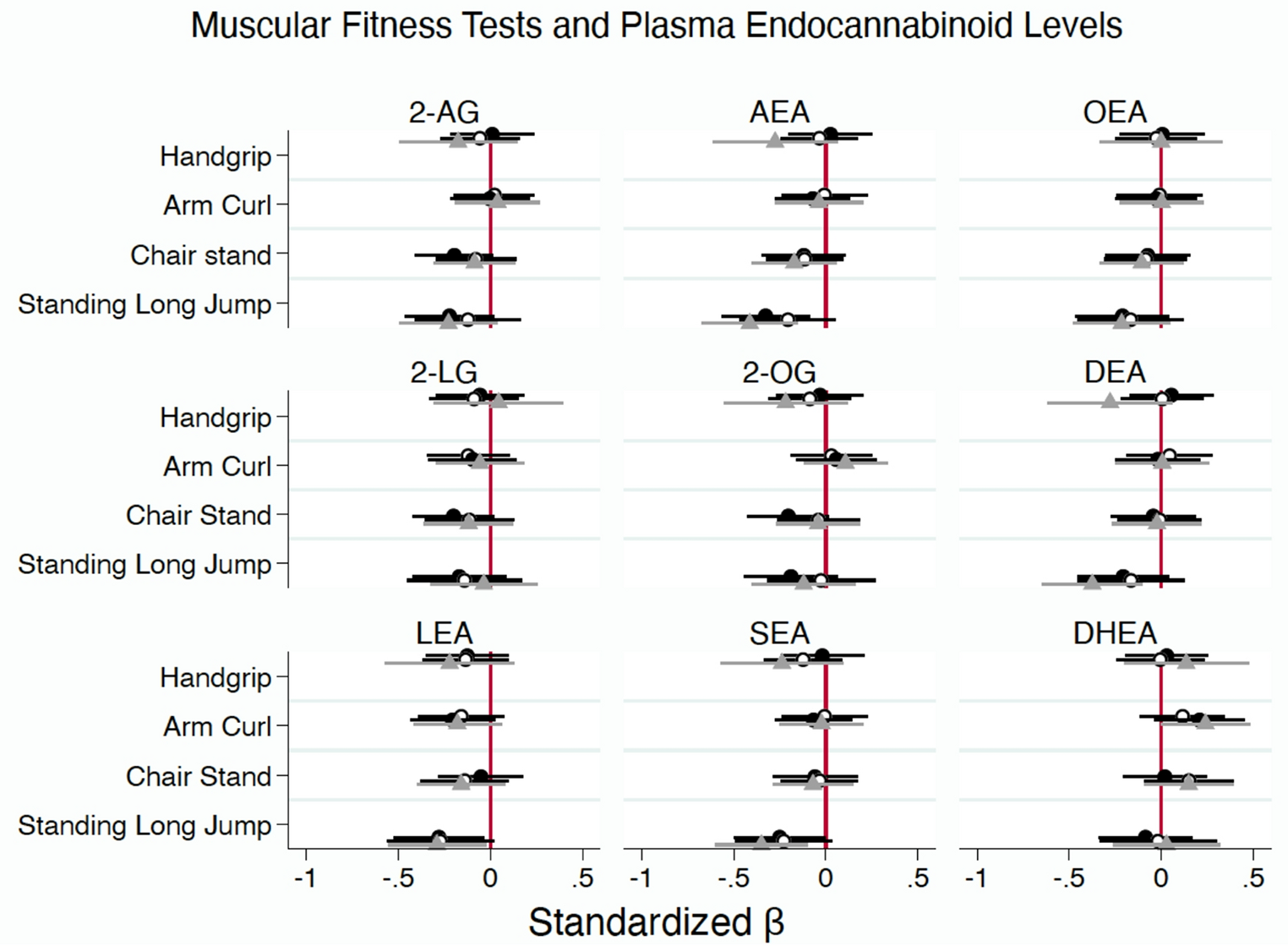
Muscular fitness (MF) Upper-limbs strength was assessed using the arm curl test, in which participants performed seated arm flexion-extension movements with a specified weight (2.3 kg for women and 3.6 kg for men), completing one 30-seconds trial per arm [34, 35]. The number of repetitions for each arm was recorded, then combined for analysis. Handgrip strength was measured with a digital dynamometer (TKK 5101 Grip-D), tested sequentially in the right and left hands, and adjusted according to each participant hand size [36]. Each hand was tested twice, and the highest value (in kilograms) from each hand was noted, with the mean of these maximum values used for analysis. Expected normative values stratified by sex and age were derived from international reference data reported by Tomkinson et al. [37].
Lower-limbs strength was evaluated using two tests. The chair stand test required participants to rise from and return to a seated position, arm crossed over the chest, as many times as possible within 30 s [38]. The total count of these repetitions was recorded. The standing long jump test was also administered to participants. They performed two maximal forward jumps from a standing start, feet together, and the greatest distance from the starting line to the nearest heel landing point was recorded in centimeters [39]. Results were compared against normative mean values for healthy adults, stratified by sex [40].
Statistical analysis
Linear regression analyses were conducted to estimate standardized (ß) and unstandardized (b) coefficients, standard errors, and 95% confidence intervals (95%IC) for the associations between fitness variables and plasma levels of eCBs and their analogues. Each fitness measure (6MWT, handgrip strength, arm curl, chair stand, and standing jump tests) was entered as an independent variable in separate models, with eCBs and their analogues concentrations as dependent variables. The Mallow Cp criterion [41] was used to identify optimal predictor variables in the regression models estimating associations for plasma levels of eCBs and their analogues with each physical fitness measure (CRF and MF test). Confounding variables were included based on their known relationship with the SE [19, 24, 42,43,44].
The analysis utilized three models. Model 1 was unadjusted. Models 2 and 3 included adjustments derived from a selection process achieving a Mallow’s Cp value of 5.00. In Model 2, adjustments were tailored to each ES biomarker: for 2-AG, 2-LG, 2-OG, DEA, and DHEA, factors such as age, BMI, and diabetes were included; for AEA, OEA, LEA, and SEA, adjustments accounted for fat mass, antidepressant medication use, and diabetes. Model 3 was identical to Model 2, except that the body composition variables (BMI or fat mass) were replaced with lean mass. Finally, we undertook a sensitivity analyses examining all associations between plasma levels of eCBs and their analogues with MF normalized to lean mass.
The assumptions of normality, linearity, and homoscedasticity were verified for all ES parameters, ensuring robustness of the regression models. Interaction effects (i.e. sex by main exposures) were considered by likelihood ratio test of nested models and by examining changes in b coefficients greater than 10%. No significant interactions were identified, permitting the analysis of all participants as a single group. Additionally, multicollinearity was assessed and found to be absent in all models; variance inflation factors (VIFs) were below 10, averaging close to 1, indicating no concern of collinearity [45]. Statistical analyses were performed using STATA version 14.0 (Stata Corp, College Station, TX, USA), with statistical significance set at p < 0.05.

Comments (0)