
Remember me
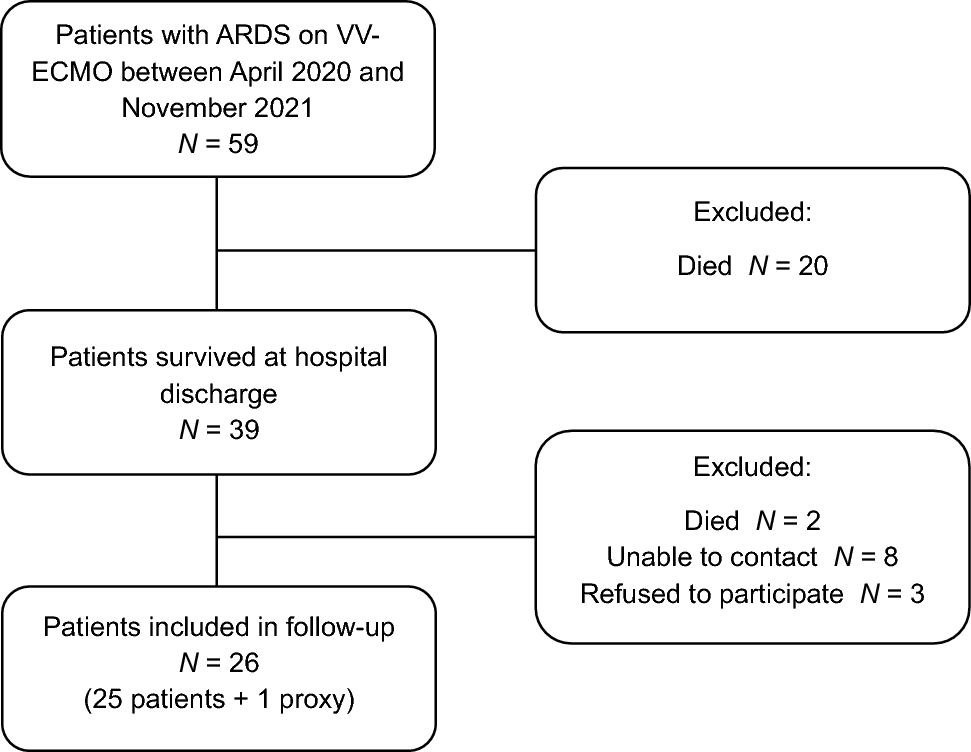
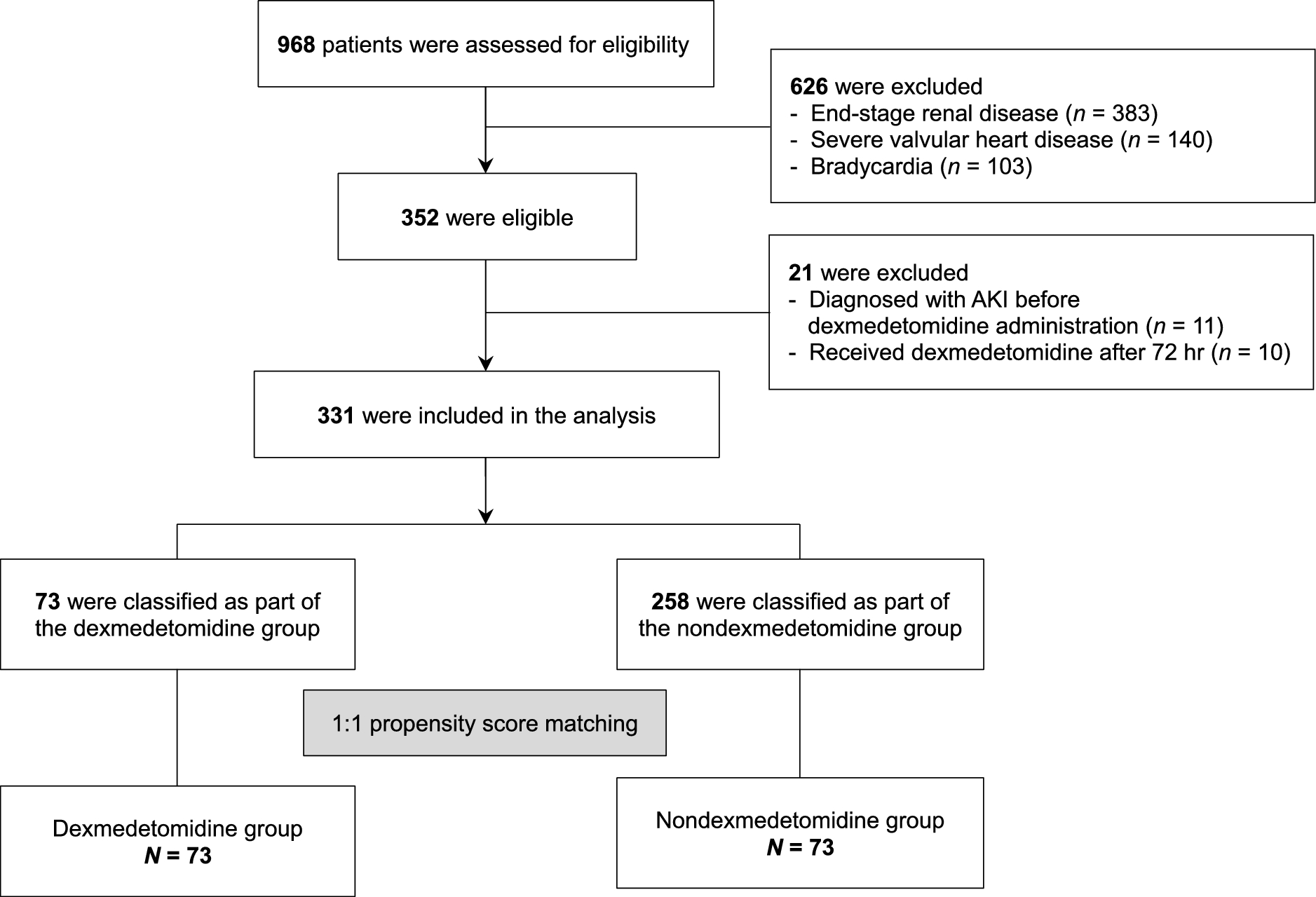
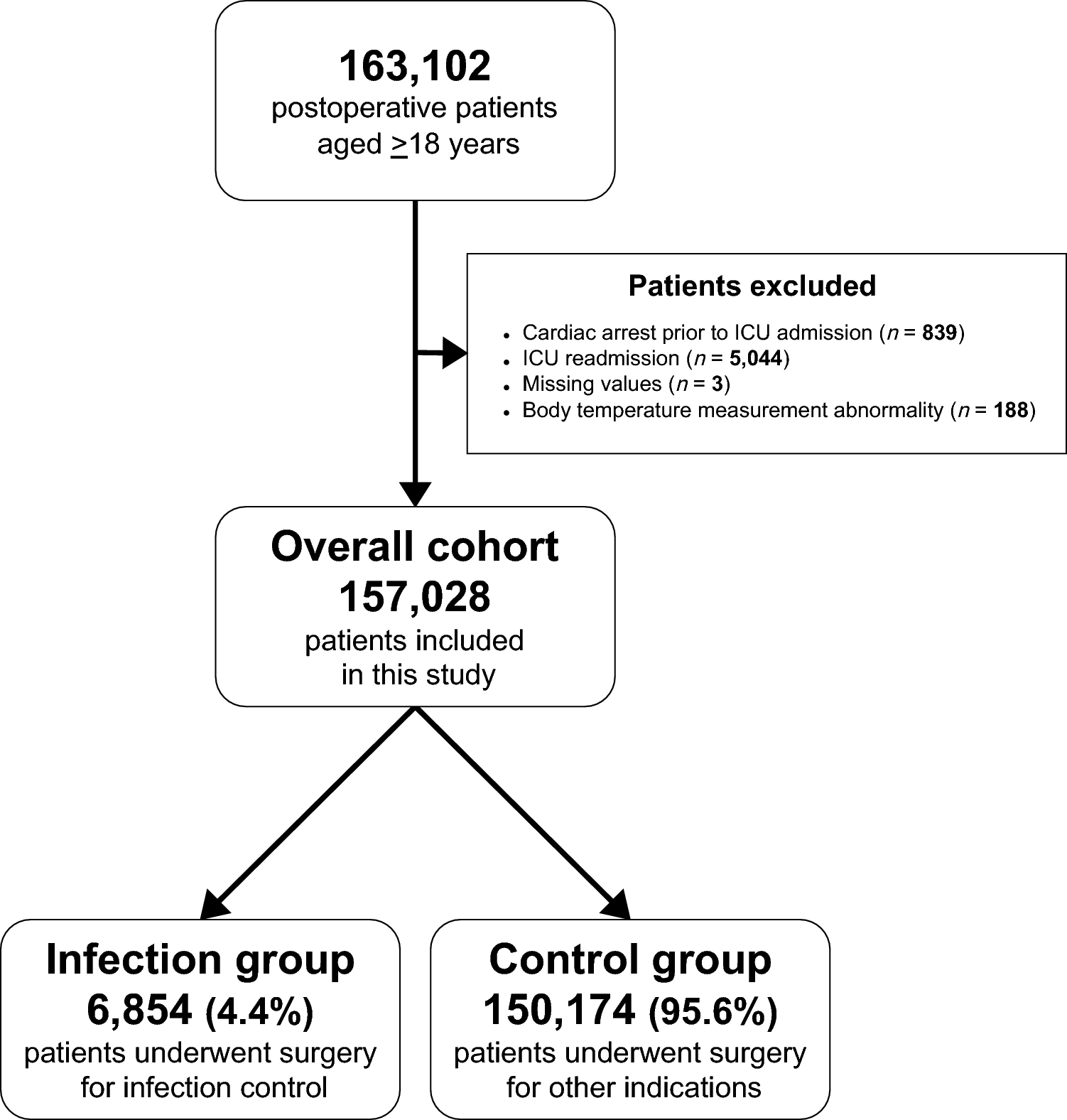
We included 331 patients in the study (Fig. 1) and classified 71 (22%) as part of the dexmedetomidine group and 331 (78%) as part of the nondexmedetomidine group. We then matched the 73 patients in the dexmedetomidine group to 73 patients in the nondexmedetomidine group using a propensity score. The median [IQR] dose of dexmedetomidine among patients in the dexmedetomidine group was 0.26 [0.20–0.40] µg·kg−1·hr−1, while no patients in the nondexmedetomidine group received dexmedetomidine. Table 1 presents the baseline characteristics of patients in the study cohorts. Patients in the dexmedetomidine group had higher median [IQR] SOFA scores (7 [4–9] vs 5 [3–8]; P = 0.002), a higher rate of cardiovascular failure (59/73 [81%] in the dexmedetomidine group vs 147/258 [57%] in the nondexmedetomidine group; P = 0.004), and higher median [IQR] blood lactate levels (2.5 [1.2–4.6] mmol·L−1vs 1.4 [0.9–2.4] mmol·L−1; P = 0.01) at the time of sepsis diagnosis. The most common sources of infection were the respiratory (125/331, 38%) and gastrointestinal (98/331, 30%) systems. The proportion of patients who underwent surgery within 48 hr prior to inclusion in the analysis was higher in the dexmedetomidine group (40/331, 55%) than in the nondexmedetomidine group (94/331, 36%; P = 0.005). There were no significant differences regarding intraoperative blood loss (median [IQR], 100 [0–625] mL in the dexmedetomidine group vs 50 [0–300] mL in the nondexmedetomidine group; P = 0.36) and blood transfusion (500 [250–1000] mL in the dexmedetomidine group vs 250 [250–937.5] mL in the nondexmedetomidine group; P = 0.10)
Fig. 1 Table 1 Baseline characteristics of patients in the study cohorts
Table 1 Baseline characteristics of patients in the study cohortsAcute kidney injury was diagnosed in 190/331 (57.4%) patients. Of these, 127/190 (66.8%), 21/190 (11.1%), and 42/190 (22.1%) patients were diagnosed with AKI stages 1, 2, and 3, respectively. The incidence of AKI did not differ between the dexmedetomidine and the nondexmedetomidine groups in both the entire cohort (54.8% vs 58.1%; P = 0.61) and the propensity-matched cohort (54.8% vs 63.0%; P = 0.31) (Table 2). Similarly, the need for renal replacement therapy (10.9% vs 9.6%; P = 0.74), ICU mortality (30.1% vs 20.1 %; P = 0.08), and 30-day mortality (32.8% vs 23.2%; P = 0.09) were not different between study groups. The median [IQR] length of ICU stay (8 [6–12] days vs 4 [2–8] days; P < 0.001) and length of hospital stay (27 [17–49] days vs 19 [9–39] days; P = 0.004) were higher in the dexmedetomidine group than in the nondexmedetomidine group.
Table 2 Study outcomes in the entire study cohort and the propensity-matched study cohortSubgroup analyses included the stratification of study groups on the basis of age, BMI, APACHE II score, diabetes mellitus, hypertension, and chronic kidney disease (CKD). In the subgroup analysis including 230 older patients (defined as age ≥ 65 yr), AKI was diagnosed in 142 (61.7%). Regarding the AKI stage, 94 (66.2%) were AKI stage 1, 14 (9.9%) were AKI stage 2, and 34 (23.9%) were AKI stage 3. Among patients aged < 65 yr, 48 (47.5%) were diagnosed with AKI. Regarding their AKI stage, 33 (68.8%) had stage 1, 7 (14.6%) had stage 2, and 8 (16.7%) had stage 3. In this patient subgroup, we observed that older patients who received dexmedetomidine had more severe disease given their higher SOFA scores and baseline lactate levels, as well as greater exposure to nephrotoxic agents and contrast media (Electronic Supplementary Material [ESM] eTable 1). Despite that, our results show that dexmedetomidine administration was associated with reduced odds of developing AKI in older patients (Fig. 2).
Fig. 2
Forest plot of the univariate subgroup analysis for acute kidney injury
APACHE = Acute Physiology and Chronic Health Evaluation; BMI = body mass index; CI = confidence interval; CKD = chronic kidney disease; Dex group = dexmedetomidine group; NonDex group = nondexmedetomidine group
We added an interaction term between dexmedetomidine administration and older patients to our multivariable logistic regression model. The model also included significant variables from univariate analysis, i.e., female sex, hypertension, diabetes mellitus, CKD, higher APACHE II score, hemoglobin levels < 10 g·dL−1, hypoalbuminemia, and administration of nephrotoxic drugs and norepinephrine (Table 3). The results of our adjusted model showed that dexmedetomidine alone was not significantly associated with a reduced AKI incidence (odds ratio [OR], 1.69; 95% confidence interval [CI], 0.60 to 1.26; P = 0.31) (Table 4). Nevertheless, we found that the interaction term between age > 65 yr and dexmedetomidine administration was significantly associated with a reduction in AKI incidence (OR, 0.25; 95% CI, 0.07 to 0.90; P = 0.03). In the propensity-matched cohort, after adjusting for covariates, including APACHE II score, hypertension, CDK, hemoglobin levels of less than 10 g·dL−1, and nephrotoxic drug administration, we also found that the interaction term between dexmedetomidine administration and older patients was statistically significant (OR, 0.17; 95% CI, 0.03 to 0.81; P = 0.02; ESM eTable 2).
Table 3 Univariate analysis of acute kidney injury from the entire cohortTable 4 Multivariable logistic regression analysis of acute kidney injury from the entire cohort
Comments (0)