Implementation of any ancillary test requires basic knowledge on whether the test is likely to yield a (reliable) result. This is especially the case when such a test comes at additional labour and monetary costs, as is the case with high-sensitivity cTn testing.
Although many studies have focused on the diagnostic value of cTn in a post-mortem setting, very little attention has been given to the variables that affect test success. For instance, the otherwise comprehensive literature review by Barberi and Van den Hondel [12] does not discuss it. Test success is briefly mentioned in the largest study up to date from Chen et al. [19], stating that haemolysis was an issue in some cases, but without providing further detail. In their 2019 review, Cao et al. suggest that frozen samples may be more affected by haemolysis and therefore should be avoided, but also without providing more data [20].
As such, our study appears to be the first which specifically focuses on variables that may influence the success of post-mortem hs-cTn testing. Our results indicate that hs-cTnI tests performed on post-mortem serum samples were overall successful and that test success is largely independent of demographic variables. A test result success of more than 75% was found in the total cohort and across the decedent demographic categories of age, sex, and BMI, in all groups with 10 or more cases.
As a rule, increased decomposition increases the probability of haemolytic or lipaemic blood samples, which both interfere with hs-cTn testing [19,20,21]. Our results confirm this, with 32 of the 34 unsuccessful tests due to degradation of the sample. Furthermore, all tests performed on decedents with visible signs of decomposition failed, although this sample was small (n = 5). We therefore advise that hs-cTnI tests should not be performed in a context of visible decomposition, although the absence of visible decomposition does not guarantee a successful test.
Lapsed time is one of the most important determinants of decomposition and our results reflect this, with an association between test success and the time between death and sample collection. Overall, success rate diminished with time, especially after a post-mortem interval of 24 h. The trajectory by which success rate diminishes is somewhat erratic, which may be explained by differences in other important determinants of decomposition, such as body temperature at time of death, circumstances at the death scene, and cause of death. The retrospective nature of our study precluded a more detailed analysis of such variables.
It was noted that test success did not differ substantially between admission and autopsy samples, even though autopsy samples are by definition taken at a later time than admission samples. This may be explained by the relatively quick turn-around-time in our institute, coupled with refrigeration of the deceased after admission. These measures are specifically taken to minimize decomposition between admission and autopsy.
The effect of time and/or decomposition on test success was also relevant to interpret the effect of sample location and CPR on test success rate. The femoral vein is the preferred location for a blood sample at VIFM, and other locations are only considered when multiple attempts for a femoral sample are unsuccessful. Often, such cases show visible decomposition, and this can explain the high level of unsuccessful tests in the low number of non-femoral samples. CPR is usually only performed in individuals with a witnessed collapse or who were last seen alive a short time before their death. By extension, the post-mortem interval and the level of decomposition can be assumed to be lower in the cohort that was resuscitated than in the cohort without resuscitation. This may explain the lower test success rate in the non-CPR cohort.
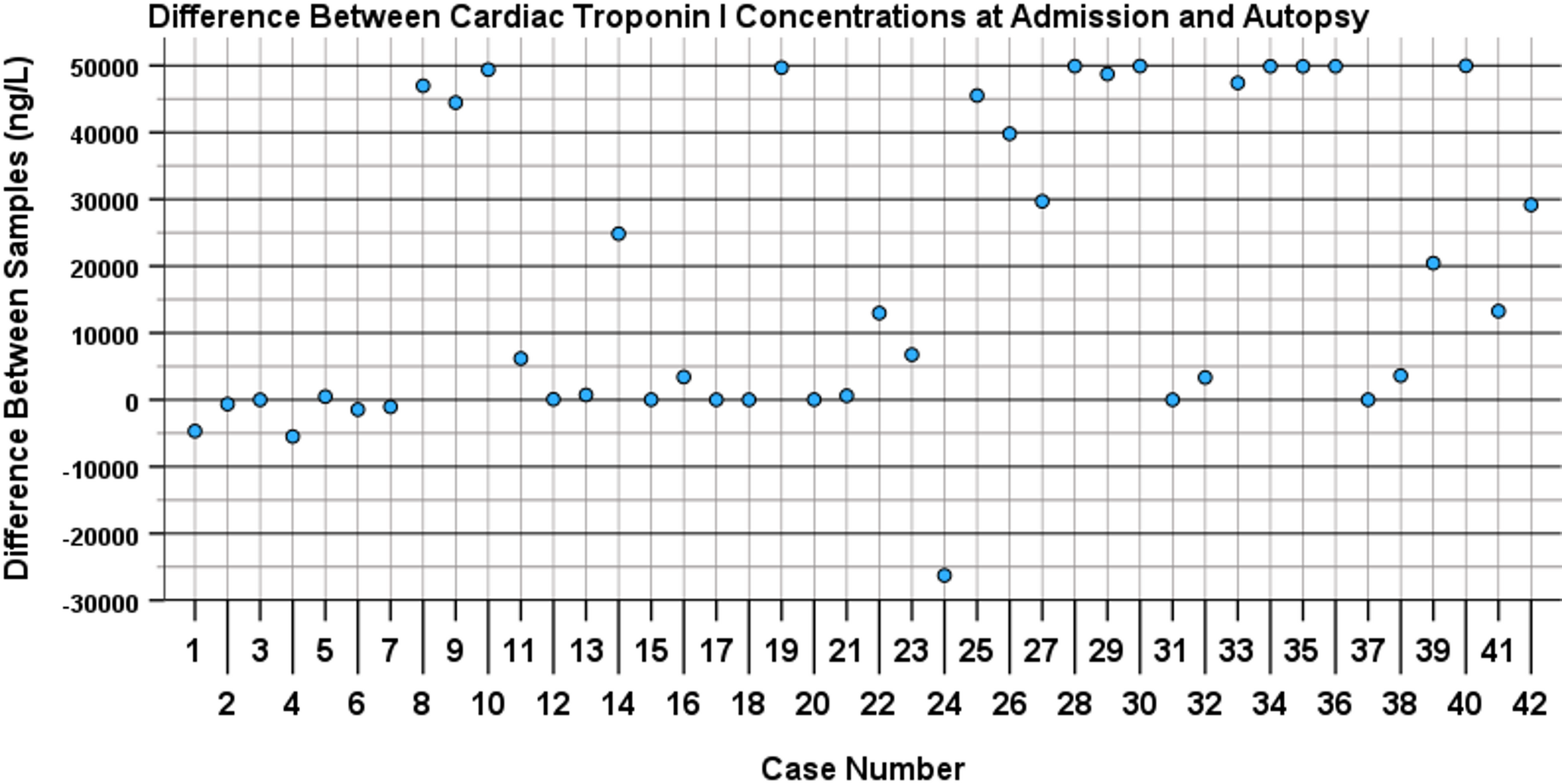
Our study demonstrated surprisingly different cTnI levels when comparing admission samples with autopsy samples from the same individual, suggesting that cTnI is very unstable in blood post-mortem. This instability did not appear to correlate with sex, age and BMI categories, in line with earlier publications [e.g., 20]. The results were erratic and difficult to interpret but overall, instability did appear to be time dependent.
The reasons for the demonstrated differences are not entirely clear. One of the proposed mechanisms is autolysis, which might cause leakage of troponin from cardiomyocytes into the blood and other tissues [22]. This would explain the increase of cTnI over time, but it cannot account for the decrease which was observed in seven out of 42 cases. Notably, almost all of the cases in which cTnI level decreased did so after a relatively short interval between admission and autopsy, i.e. less than 36 h.
Comparison of our results with previous work is challenging since the literature on post-mortem stability of cTnI or cTnT is conflicting. This was already noted by Palmiere et al. in 2018 [22],, who summarized the literature on the subject, and stated that Zhu et al. [14, 23, 24], Remmer et al. [25], and Chen et al. [19] found time-dependent differences in post-mortem troponin levels, while Pérez-Carceles et al. [26] and Peter et al. [27] did not. The study of Gonzales-Herrera [28] also found a time-dependent increase. These studies all have methodological limitations though. They did not, like the current study, test two samples from the same person at different points in time. Rather, they inferred stability from comparing results between selectively included cases which were stratified according to post-mortem interval. Our methodology and results reflect that of Moridi et al. [13] who compared high-sensitivity cTnT test results at admission and autopsy and found significant differences between them. Combining our results with the existing literature, we conclude that there is considerable evidence to suggest that cTnI and cTnT are markedly unstable in post-mortem blood under normal operational conditions at our Institute, especially with increased PMI.
Whether this instability is relevant depends on how a hs-cTn result is interpreted. It is generally agreed upon that ‘normal’ post-mortem levels of cTnI are much higher than ante mortem levels, and that the clinical cut-off value (the 99th percentile) of 40 ng/L [29, 30] has no relevance in a post-mortem setting. An alternative cut-off value has not been agreed on. Such a cut-off value is likely to depend on the specific diagnostic issue and circumstances of the case.
It has been suggested that frozen blood samples should be avoided for biochemical analysis (Cao et al., Barberi et al.) due to the likelihood of haemolysis. Our institute uses frozen serum samples, not whole blood samples. This should prevent further haemolysis once the serum sample is obtained. Storage of the serum samples at -20 directly after centrifuging, and only defrosting a sample for analysis aims to further limit degradation. The defrosting and refreezing required for transportation could theoretically have affected stability, but our study design was unable to examine this in more detail. Various other studies also used frozen serum samples, apparently without major issues (e.g [9, 10, 31, 32]).
To confirm whether cTnI levels indeed remain stable in serum at -20 degrees Celcius, we attempted to compare the subset of older (retrospective) cases with cases with limited serum storage time (prospective cases). An unfortunate and unexpected clustering of cases in terms of post-mortem interval however precluded this sub analysis. The use of older frozen samples cannot always be avoided, since the need for a hs-cTn test may not be readily apparent at the time when the sample is taken. Further research is therefore needed to determine if storage at -20 degrees Celsius indeed limits further degradation of the sample.
Our study has several limitations. First, it was performed in the context of normal operations at our institute. As a consequence, many variables were deliberately unaccounted for. For instance, we did not selectively include decedents with a specific PMI, and we did not regulate the amount of time between blood samples or laboratory processes in Part B of the study. This hampered interpretation of some of the results. For instance, minor variability in the time between obtaining and centrifuging blood samples could theoretically have confounded our results on cTnI stability. At the same time, conducting our research in the setting of normal operations ensured our results are representative of (and applicable to) our daily practice. The workflow in our institute is likely similar to many large forensic pathology institutes, making the results also transferrable to their situation.
Another limitation related to sample size. Sample sizes were dependent on inherent financial, operational, and time constraints, resulting in low case numbers in some subcategories. For example, the 10–19, 20–29, 30–39, 90–99 age groups and the underweight BMI category were underrepresented in the data. Future research is needed to address this.
Lastly, our only studies focused on cTnI, as cTnT testing is not available at our institute. It is assumed that many of the processes that affect the availability and stability of cTnI are the same for cTnT, but this has not been confirmed experimentally.

Comments (0)