This study showed that traumatized rBM exhibits a specific and time-dependent proteomic response following rib fractures. A significant overexpression of acute-phase proteins, extracellular matrix components, and bone-specific proteins was observed in the trauma group compared to controls. These findings support the concept of rBM as a dynamic tissue capable of revealing vital reactions even within short survival times.
Many proteins belonging to the acute phase such as factors of the complement activation, coagulation and hemostasis were identified. These proteins also increased over the survival time along with the magnification of the inflammation, as demonstrated by the functional analysis (biological pathways). Hemostasis and coagulation proteins initiate the fracture healing process by forming a fibrin clot, which stabilizes the injury site and provides a matrix for cellular infiltration [6]. These proteins also release signaling molecules that recruit immune and progenitor cells. The complement system, activated early after injury, modulates inflammation, enhances phagocytosis of debris, and promotes osteogenic cell recruitment and differentiation [19]. Together, these systems start to orchestrate the transition from inflammation to tissue regeneration during bone repair [10].
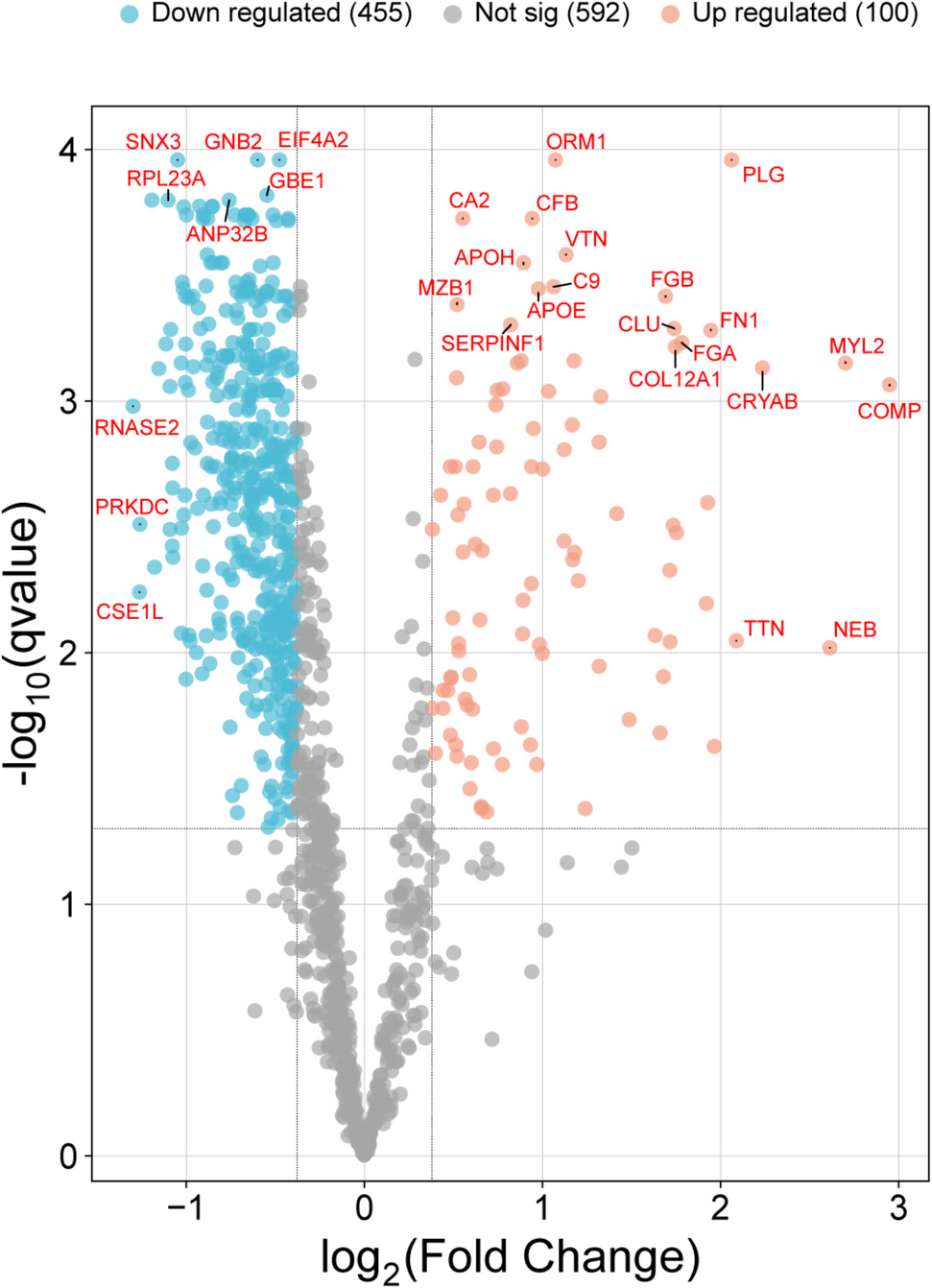
Interestingly, rBM overexpressed, especially in the first 24 h after trauma, several complement factors of both the classic and alternative pathways at different levels and with high statistical significance, which suggests that this biological process can be referred as a general condition of vital reaction. Noteworthy, some of these proteins showed very interesting patterns such as complement C9 which provided the best significant results over time, according to its biological functions. Thus, C9 is a terminal component of the complement system, forming the membrane attack complex (MAC). In fracture repair, C9 contributes to the clearance of pathogens and damaged cells, indirectly supporting a controlled inflammatory environment necessary for bone regeneration [20]. Furthermore, fibrinogen statistically increased starting from 4 h after trauma; beyond its pathophysiological role in hemostasis, fibrinogen provides a scaffold for cell migration and releases bioactive peptides that modulate inflammation and promote osteoblast differentiation [21].
The proteomic analysis also demonstrated a pivotal role of proteins belonging to extracellular matrix organization, cell adhesion, cytoskeletal organization and collagen fiber assembly. rBM significantly overexpressed collagen VI starting from the first hours after injury, with a marked increment after 24–48 h. During fracture repair, it forms the organic matrix of the callus, guiding mineralization and providing mechanical strength. It also influences cell adhesion, migration, and differentiation of hematopoietic elements for the acute phase [22]. Collagen XII, decorin, tenascin, vitronectin, and COMP were also upregulated but pose more specific pathophysiological considerations. Noteworthy, collagens and other ECM proteins participate in the establishment of the primary soft callus which gradually substitutes the hematoma [6, 9, 10]. This finding corresponds to the results of the current research and highlights a fluid cooperation of different proteins (APPs and ECMPs) in the bone healing process. Therefore, these ECM proteins can be considered as suitable rBM markers of early lesion reaction in the forensic setting since they show significant increases over time with only selected expressions among other tissues.
rBM overexpressed after traumatization high-specific proteins related to bone metabolism which include carbonic anhydrase 2, alpha-2 HS-glycoprotein, vitamin D-binding protein, and COMP. CA2 also showed an interesting parabolic trend with an increment over the first 12 h and likewise a decrement up to 96 h after trauma, as shown in Fig. 4D. This enzyme is one of sixteen forms of human carbonic anhydrases [23]. Carbonic anhydrase catalyzes reversible hydration of carbon dioxide and interacts with band 3 anion transport protein. Defects in CA isoform 2 are associated with osteopetrosis, cerebral calcifications and renal tubular acidosis [24]. Specifically, CA2 deficiency is the paradigm osteopetrosis featuring failure of osteoclasts to resorb bone due to inability to acidify their pericellular space [25]. CA2 loss-of-function leads clinically to bone fragility and pathological fractures. Furthermore, bone healing in individuals suffering from osteopetrosis is impaired [26], thus suggesting a central role of CA2 in this biological process.
On the other hand, AHSG is a fetuin protein which still shows obscure roles. However, it can inhibit calcification as well as osteogenesis in bone [27]. Furthermore, osteoclasts are stimulated by GC [28]. According to these considerations, rBM immediately starts to upregulate some highly specific proteins related to bone metabolism to promote the osteoclastic resorption of injured hydroxyapatite with a maximum peak at 12 h after trauma. This finding is of utmost importance since it postulates that CA2, SLC4 A1, and AHSG may be useful to distinguish early vital reactions in bone tissue due to the activation of osteoclasts in the context of bone turnover.
Before concluding, bioinformatic analysis revealed two important proteins which are used in routine forensic pathology for vitality definition such as glycophorin A (GLYA) [29,30,31] and aquaporin-3 (ACQ3) [1, 32, 33]. However, they did not show a statistical significance between the trauma group and the controls. Similarly, many proteins involved in the mechanisms of adhesion (ICAM3, MCAM, NCAM1, PECAM1, and VCAM1) [34] were not identified as significant, thus imposing great caution in their use on bones as markers of vital reaction.

Comments (0)