In this study of chemotherapy-naïve mHSPC patients treated with abiraterone or apalutamide as first-line therapy in routine clinical practice, apalutamide was associated with a profound and more sustained PSA reduction compared to abiraterone, which translated into delayed disease progression. Both treatments were well tolerated, although a higher prevalence of adverse events was observed in the apalutamide cohort.
Low PSA levels during initial treatment have shown significant correlations with improved survival and clinical outcomes [11, 12, 20]. PSA50, PSA90, PSA ≤ 0.2 and PSA ≤ 0.02 rates were significantly higher in the apalutamide cohort at the first month follow-up compared to the abiraterone cohort. However, no statistically significant differences were observed in the other follow-ups regarding PSA50 and PSA90. Previous research had also observed no evidence of improved PSA90 rates at the 12-week follow-up in mHSPC patients between apalutamide, abiraterone and enzalutamide [14, 16], although Lowentritt et al. [15] did found a higher percentage of patients achieving PSA90 at 6- and 9-months follow-up in the apalutamide cohort. Moreover, apalutamide showed a higher proportion of patients achieving PSA levels ≤ 0.2 ng/ml and ≤ 0.02 than abiraterone at every time measured, also observed in previous observational studies where both apalutamide and enzalutamide showed similar results compared to abiraterone [14, 16], which was translated into a longer time remaining with ultralow PSA level. Although the abiraterone cohort had higher baseline PSA levels, similar results were observed in other studies with unbalanced PSA characteristics [14, 16] supporting the consistency of our findings. These results indicate that while both treatments are effective in reducing PSA levels, apalutamide achieves a deeper and more rapid PSA reduction, which is sustained for a longer duration compared to abiraterone, consistent with previous research.
In our study, the PSA nadir was significantly lower in the apalutamide cohort, with a median value of 0.02 [0.02–0.04] ng/mL, comparable to findings from both the TITAN trial population and other real-world studies [7, 14, 21]. Additionally, a shorter time to PSA nadir was observed in the apalutamide cohort. Wenzel et al. [13] observed that the proportion of mHSPC patients achieving a PSA nadir of ≤ 0.02 was significantly higher in the apalutamide cohort versus the abiraterone cohort. However, Lu Yutong et al. [14] patients did not find statistically significant differences in PSA nadir or time to nadir, although PSA values were lower on the apalutamide group, possibly due to the low number of patients included in this study.
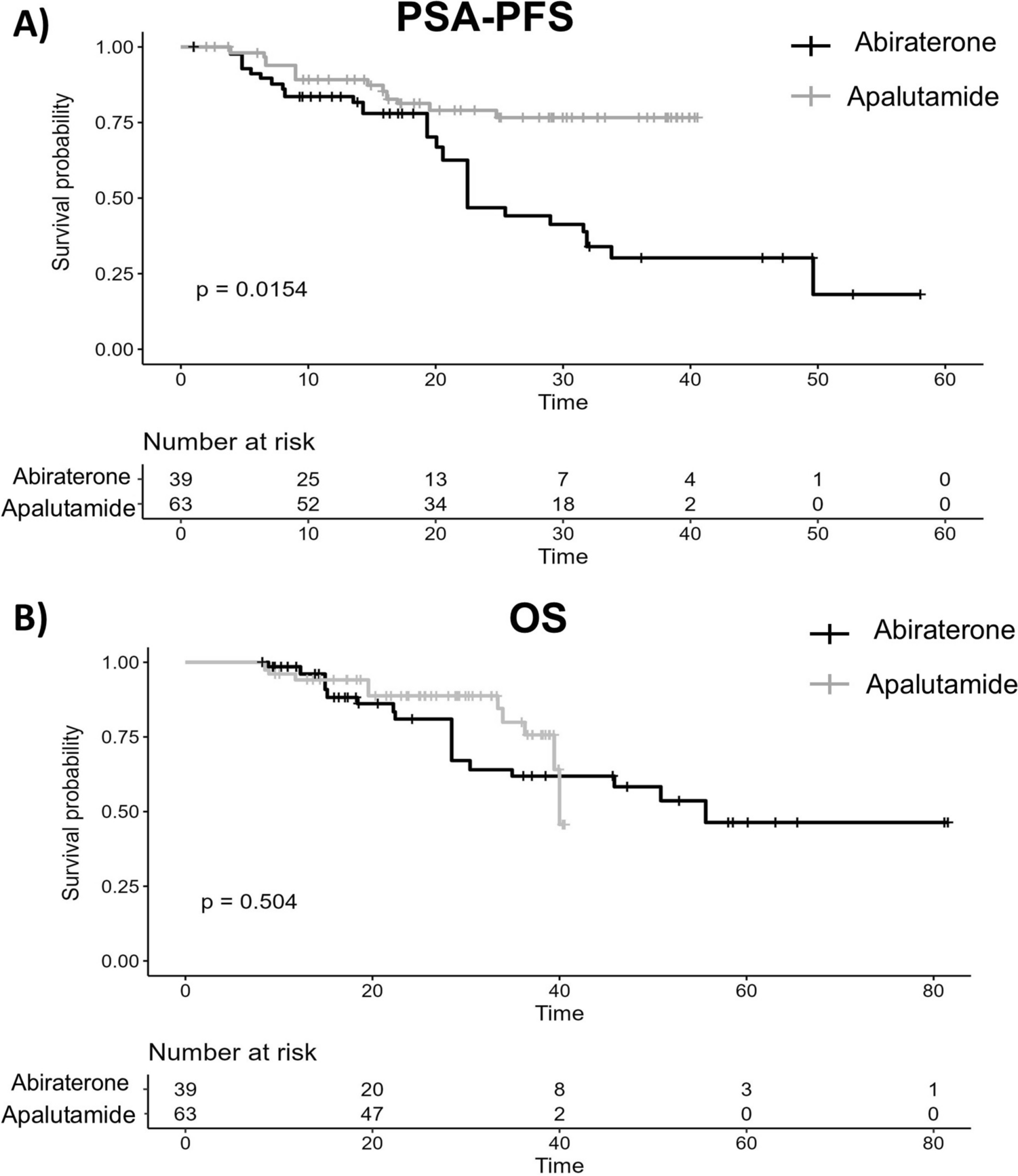
Recent research indicates that achieving PSA levels below 0.02 ng/mL at any point during combination therapy confers substantial, statistically significant, and long-term benefits in OS and disease progression control [13, 22]. Furthermore, in a post-hoc analysis of the TITAN trial, PSA thresholds of ≤ 0.2 ng/mL and ≤ 0.02 ng/mL were associated with significantly longer rPFS, OS, time to PSA progression, and CRPC-PFS [12]. In our study, apalutamide showed a favorable PSA-PFS compared to abiraterone, demonstrating a significant advantage in delaying disease progression, consistent with other observational studies [13, 14]. Moreover, patients achieving PSA50, PSA90, PSA ≤ 0.2 and PSA ≤ 0.02 at any point during the study period as well as treatment with apalutamide appeared as protector factors in the univariate Cox regression analysis. However, only achieving ultralow PSA levels was associated with delayed progression in the multivariate analysis, having a 93% less risk of disease progression. Similarly, Wenzel et al. [13] observed that patients who achieved PSA nadir of ≤ 0.02 ng/mL with apalutamide had the best outcomes in terms of time to castration resistance and OS rates. Regarding OS, no statistically significant differences were observed between groups, as previously observed in other real-word studies [14, 16]. However, our OS results should be handled with care due to the low number of deaths and the influence of subsequent treatments, as can be seen in a higher percentage of abiraterone patients treated with docetaxel after progression, which could bias the results. Overall, these findings demonstrate a strong association between achieving ultralow PSA levels and delayed disease progression.
The safety profile of ARATs can also influence drug selection. A recent meta-analysis of randomised controlled trials assessing the adverse events associated with ARATs found a higher risk of high blood pressure and headache risk in patients treated with enzalutamide but no significant difference in adverse event rates between apalutamide and abiraterone [23]. However, in our study, a higher prevalence of adverse events was observed in the apalutamide cohort, with fatigue being the most common side effect, followed by skin rash. In a retrospective comparison of abiraterone, enzalutamide, and apalutamide, Suzuki et al. [16] reported a higher prevalence of grade 3 adverse events in the apalutamide cohort, with skin rash being the most frequent. Factors such as a broader and more heterogeneous population, more flexible monitoring and reporting standards, and variations in adherence could explain the differences observed between clinical trials and real-world data. Overall, both treatments were reasonably well-tolerated, with no adverse events leading to death and a low percentage of patients discontinuing treatment due to adverse events.
The findings of our study should be interpreted within the limitations of data and study design. Firstly, its single-centre and retrospective design restricts generalizability and may also introduce biases in data collection and reporting. Additionally, the retrospective nature limited our ability to prospectively power the study for several key endpoints (PSA kinetics, overall survival), potentially resulting in analyses underpowered to detect small but clinically meaningful effects. Secondly, considering the regression models for IPTW, it is important to highlight that unobserved baseline characteristics and confounders may remain unaccounted for, potentially leading to hidden imbalances in the index-treatment cohorts, even after applying IPTW. Moreover, baseline PSA was not fully balanced, which could result in an overestimation of the present findings. Thirdly, no data on dosage or dose reductions were available for inclusion in our analysis, which may have influenced the results. Despite these constraints, to our knowledge, this is the first study to provide an in-depth comparison of PSA dynamics between abiraterone and apalutamide treatments, addressing limitations in prior studies that either had very small patient cohorts, examined few variables, or did not adjust for baseline differences between groups, providing useful information for optimizing treatment strategies in mHSPC.

Comments (0)