Study design and settings
This prospective observational cohort study was conducted across four EMCC in France from January 22nd to March 7th 2024. In the French EMCC system, incoming calls are initially managed by a call taker who records the caller’s identity and the reason for assistance. If dyspnea is identified as the chief complaint, the call will be transferred to an emergency physician for medical evaluation and regulation. He or she will conduct a thorough medical interview to assess the patient’s condition and determine the appropriate intervention, which may include either medical advice or first-aid team dispatch. This team may include an basic life-support ambulance, or a Mobile Intensive Care Unit (MICU) staffed with a physician and nurse, depending on the patient’s severity. The decision-making process regarding the dispatch of these units is not protocolized and varies across all EMCC. The decision is based on the physician’s clinical discernment to decide whether to dispatch a MICU if respiratory distress is identified during the call. Following the initial deployment of the first-aid team, the EMCC subsequently coordinates with hospitals to settle the patient’s transfer, taking into account both the patient’s medical requirements and the current capacity of nearby healthcare facilities [11]. In France, MICU are the only prehospital team able to provide respiratory support such as high-flow oxygen, NIV, manual and mechanical ventilation after intubation. Patients transported by paramedics without MICU will benefit from such support at the ED arrival if necessary.
Participants
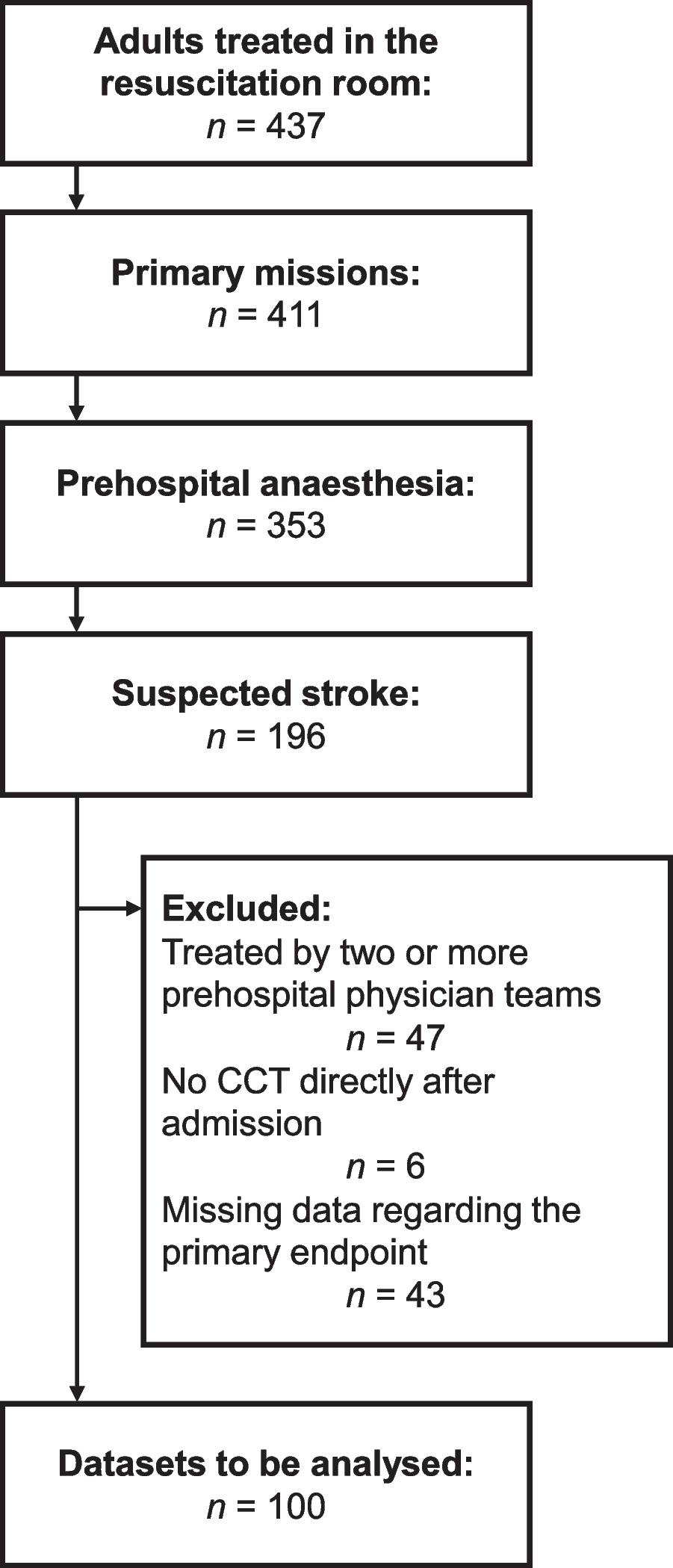
Patients over the age of 18 years that called the EMCC once for acute dyspnea (< 7 days) were included. Exclusion criteria were: cardiac arrest during the initial call, patients identified as not-to-be-resuscitated, special circumstances (i.e. traumatism or anaphylaxis) and patients that refused to participate. This study has been registered by the University Hospital of Toulouse in line with the French MR-004 Methodology (CNIL number: 2206723 v 0; Institutional Register Number: RnIPH 2023-87).
Primary end-point and variables
The primary endpoint was an immediate respiratory support (i.e. high-flow oxygen, NIV, manual or mechanical ventilation after intubation) prior to hospital registration (initiated by MICU) or at ED registration (within the first hour after registration). Patients that died before arriving to the hospital were also considered as presenting the primary endpoint.
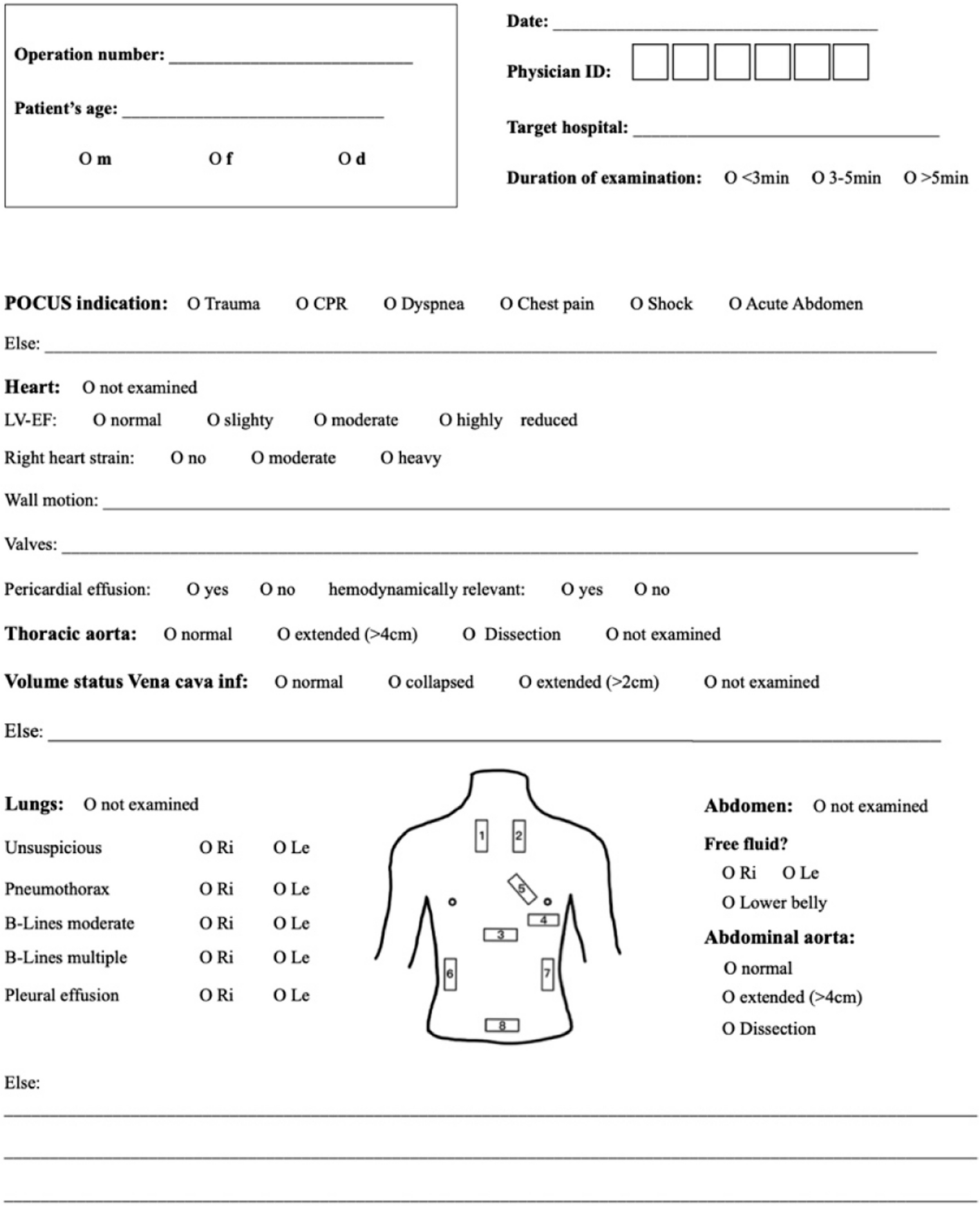
Variables of interest to predict respiratory support were prospectively collected in the EMCC by the Emergency Physician (EP) during the first medical interview. During this call, EP were requested to collect patients’ usual treatment (especially furosemide and β2-mimetics), dyspnea duration before call, if patients presented tachypnoea, abnormal respiratory noises, inability to speak full sentences, cyanosis, sweats, abdominal respiration or altered consciousness [5]. If possible, self-report breathing discomfort was collected using a numerical scale from 0 (no discomfort) to 10 (worst breathing discomfort imaginable) [10]. The EP intuition on the risk of immediate respiratory support was also collected on a scale from 0 (no risk) to 10 (the patient is very likely to need respiratory support immediately). Parameters at first contact, pathway after ED, 7-day mortality and final diagnosis after discharge were also collected from hospital charts if possible (i.e. if patients had/presented a first contact with at least an ambulance and eventually was taken to a hospital).
Study size
Based on findings from a preliminary study [5], we hypothesised that 10 to 15% of patients would require immediate respiratory support. With 1000 patients, we could have identified between 100 and 150 that may have required immediate respiratory support. We initially planned to split the cohort in two groups for development (2/3) and internal score validation (1/3). This number of inclusions should allow us to explore between 7 and 10 potential predictors in the derivation cohort, considering that multivariate analysis requires 10 events per variable included in the model. During the 1.5 month of inclusion, we managed to include 652 patients. In the absence of fundings, the study could not be extended any further. Conservatively, we finally developed one predictive score with no internal validation.
Statistical analyses
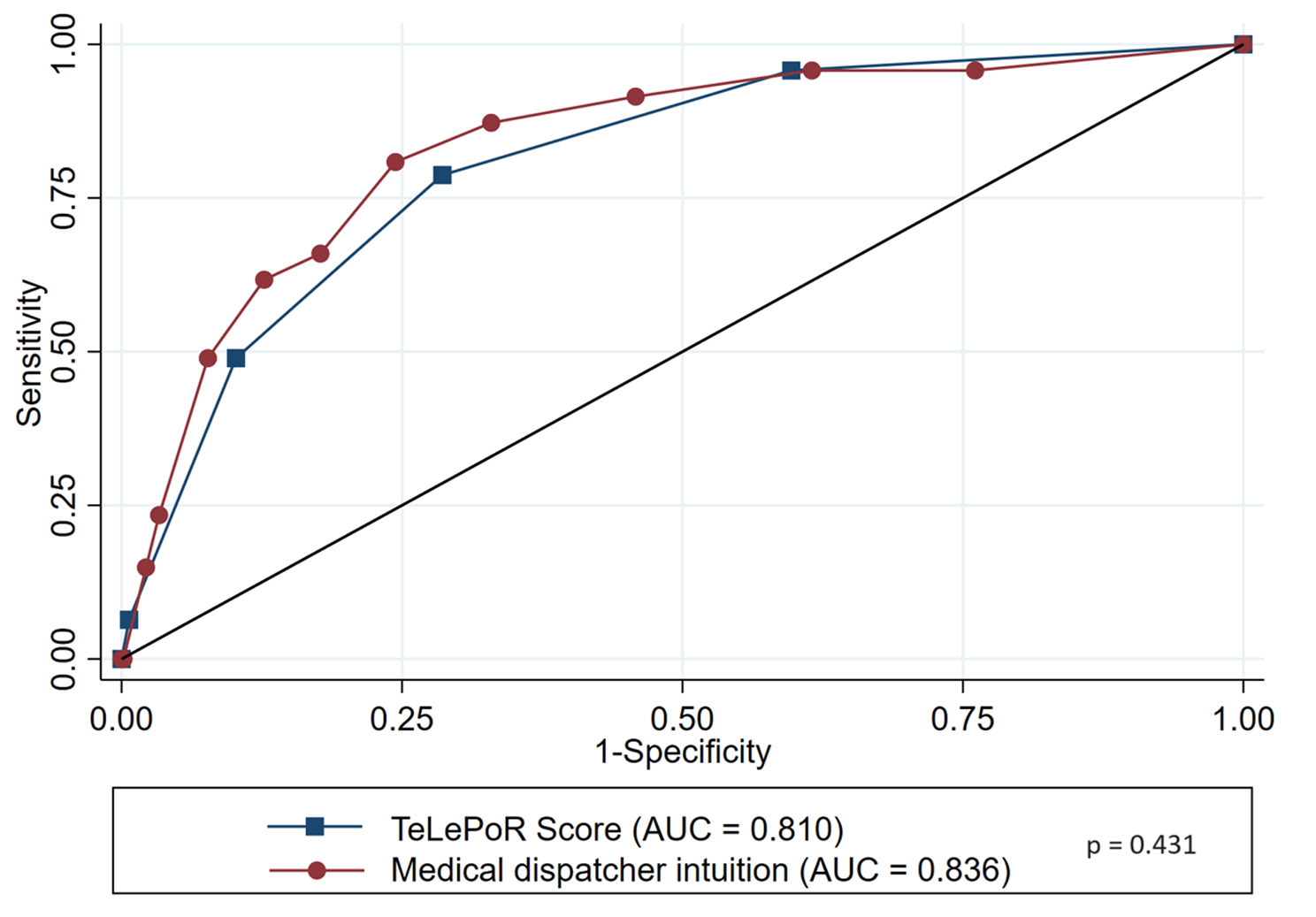
Data were analysed with STATA software (version 16; StataCorp, College Station, TX). No imputation was used in order to describe the population. Quantitative variables were described with median and IQR (m (q1-q3)) and Mann-Whitney test was used to compare groups. The threshold for self-report breathing discomfort was chosen using Liu cut-point method to maximise both sensitivity and specificity. Qualitative variables were described with number and percentage (n(%)). Moreover, Chi2 or exact-Fischer test was used to compare groups. To identify predictive factors of immediate respiratory support, we used stepwise logistic regression. Missing values regarding potential predictors were considered as normal. The final multivariate analysis only showed risk factors remaining associated with p-value < 0.05. A scoring system was therefore developed (the TeLePhon Respiratory Score (or Toulouse-Lyon-Poitiers-Renne Score) (TeLePoR Score), based on the risk factors identified. The test characteristics (i.e. sensitivity, specificity, positive and negative predicting values) of TeLePoR score were also calculated with their 95% confidence interval (95%CI) for every threshold. Afterwards, the score performance was compared to medical dispatcher’s intuition.


Comments (0)