During procedural sedation with RM administered by emergency medicine physicians or nurse anaesthetists, two out of 103 patients experienced severe respiratory adverse effects that could be effectively treated in the emergency department. Patients were safe to leave unsupervised after a median of 15 min in both groups, and procedural success was high in both groups.
In this pragmatic clinical study, the incidence of any adverse events is reported. Many patients received opioids during the procedural sedation with RM (26% in group 1/emergency medicine physicians and 18% in group 2/nurse anaesthetists).
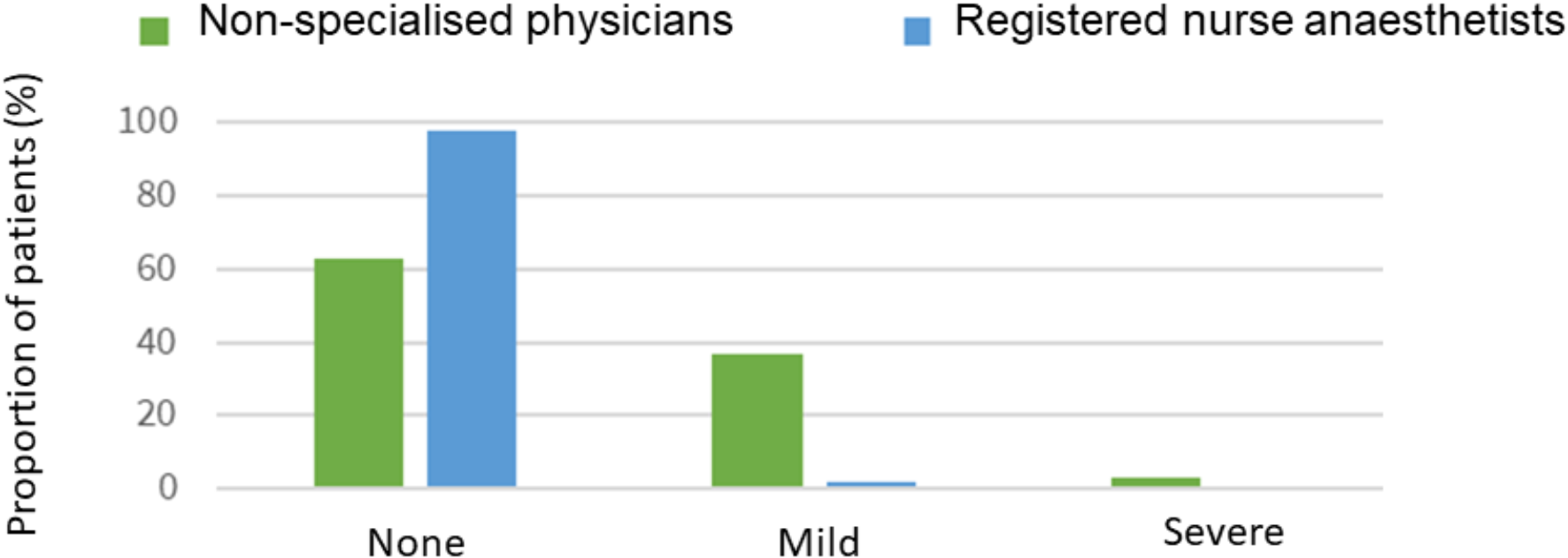
Only two patients developed severe respiratory adverse effects, and in both patients, symptoms could be resolved in the emergency department by simple airway manoeuvres, bag-valve-mask ventilation for a short period of time and/or administration of an antidote. These procedures are all well known by the staff in E.Ds. The proportion of patients requiring a manual airway manoeuvre is lower than in a recent prospective observational study of adult patients receiving RM in an ED in the Netherlands [15].
Amnesia was reported in most patients which is desired for patients undergoing painful procedures. While most patients showed objective signs of pain during the procedure, this had minimal impact on their overall satisfaction, as nearly all patients had amnesia for the procedure. These findings are consistent with those of Yao et al., who also reported a high patient satisfaction after sedation with RM during colonoscopy [16].
There were positive experiences with all attempted procedures. Several of the colleagues, who performed the painful procedures on the patients, expressed ability to more easily perform the procedures. They attributed this to their experience of improved sedation, better patient relaxation, and reduced time consumption due to easier adjustment of sedation and anesthetic depth. However, data has not been collected regarding this. Providers expressed confidence in the safety of administering RM [16, 17].
Time from first dosage until 87% of emergency medicine physicians without anaesthesiologic specialisation and 88% of registered nurse anaesthetists could safely leave patients unsupervised was less than 20 min. Our findings on the rapid onset and recovery times are consistent with an existing study on the sedative effect of RM [17]. The rapid recovery time and no active metabolites makes RM useful in the ED, as patients can be discharged earlier than after general anaesthesia.
Sancheti et al. states the following essential properties for sedatives: rapid onset, short half-life and pharmacologic reversibility, minimal impact on cardiac and respiratory function and lack of accumulation with sustained use as well as reliance on a particular organ metabolism [18]. The abovementioned properties were consistent with our findings concerning the safety and effectiveness of RM. The ED treats a diverse patient population with various comorbidities, enhancing the generalisability of our findings to other settings. However, in our opinion, it is essential that the setting has an on-call anaesthesiologist.
Strengths and limitations
The study was conducted in a non-randomised clinical setting with consecutive patient inclusion, where the assignment to nurse or physician was based on provider availability during shifts. No formal power analysis was conducted, as this was an observational study based on the availability of patients receiving Remimazolam in our ED during the study period. All patients undergoing procedural sedation with RM during the study period were included, which minimised selection bias during the inclusion process. Providers were attending clinical duty during the inclusion and sedation of the patients. While this design offers certain advantages, it has notable limitations, particularly the lack of comparison to “standard care” scenarios, such as sedation in the emergency department using Alfentanil + Midazolam or nerve blocks and admission to an orthopaedic department while awaiting operating room availability Another limitation is that, due to the real-world nature of this study, a strictly matched-cohort analysis was not feasible.
A notable limitation is that patient satisfaction was assessed by the administering provider, potentially introducing treatment provider bias and a response bias. Additionally, the outcome “provider experience” is susceptible to outcome-assessor bias, as the same individual who performed the procedural sedation also evaluated their own experience.


Comments (0)