In recent years, mobile ultrasound has increasingly found its way into emergency medicine as a useful and important tool for detecting serious problems bed-side respectively on scene. The work presented here examines POCUS use in prehospital care in Germany and the need for EMS physician’s education to perform adequately.
Our data shows a wide range of indications for POCUS examinations in various leading symptoms relevant to emergency medicine. Already established in trauma patients [13], ultrasound also appears to be able to provide findings for prehospital care in many internal medical conditions too, especially by examining the heart and lungs.
Participants used mobile hand-held ultrasound devices focused on answering certain questions on scene. All examinations took less than 5 min. This time span was also demonstrated in other studies, so time on scene was not significantly extended in operations in which ultrasound examinations were performed prehospital [14]. This alleviates concerns about delays in patient care when using prehospital emergency POCUS. Regarding all this, our results are comparable to those from recent years [1, 3, 5, 15,16,17,18,19,20,21,22].
A research group from Switzerland investigated the distraction caused by ultrasound examinations of critically ill patients. They found a significant decrease in oxygen saturation went unnoticed in 75% of cases when ultrasound was used caused by focusing on POCUS examination during patient’s care. This result should be taken into account when considering whether ultrasound provides an advantage in treatment [23]. Despite the fact that on scene time is not significantly affected, ultrasound examination can distract the emergency physician`s focus, especially the inexperienced, from upcoming serious patient’s problems and immediate treatment.
Looking at the course of the patient, it was found that in addition to early diagnosis and thus more targeted therapy, the length of hospital stay of patients who have undergone prehospital sonography is shorter than that of patients who have not had an ultrasound examination which demonstrates a clear advantage of prehospital ultrasound [23].
From the author’s point of view, these data underline the important role POCUS has found in becoming an integral part of prehospital care, so it should be used universally.
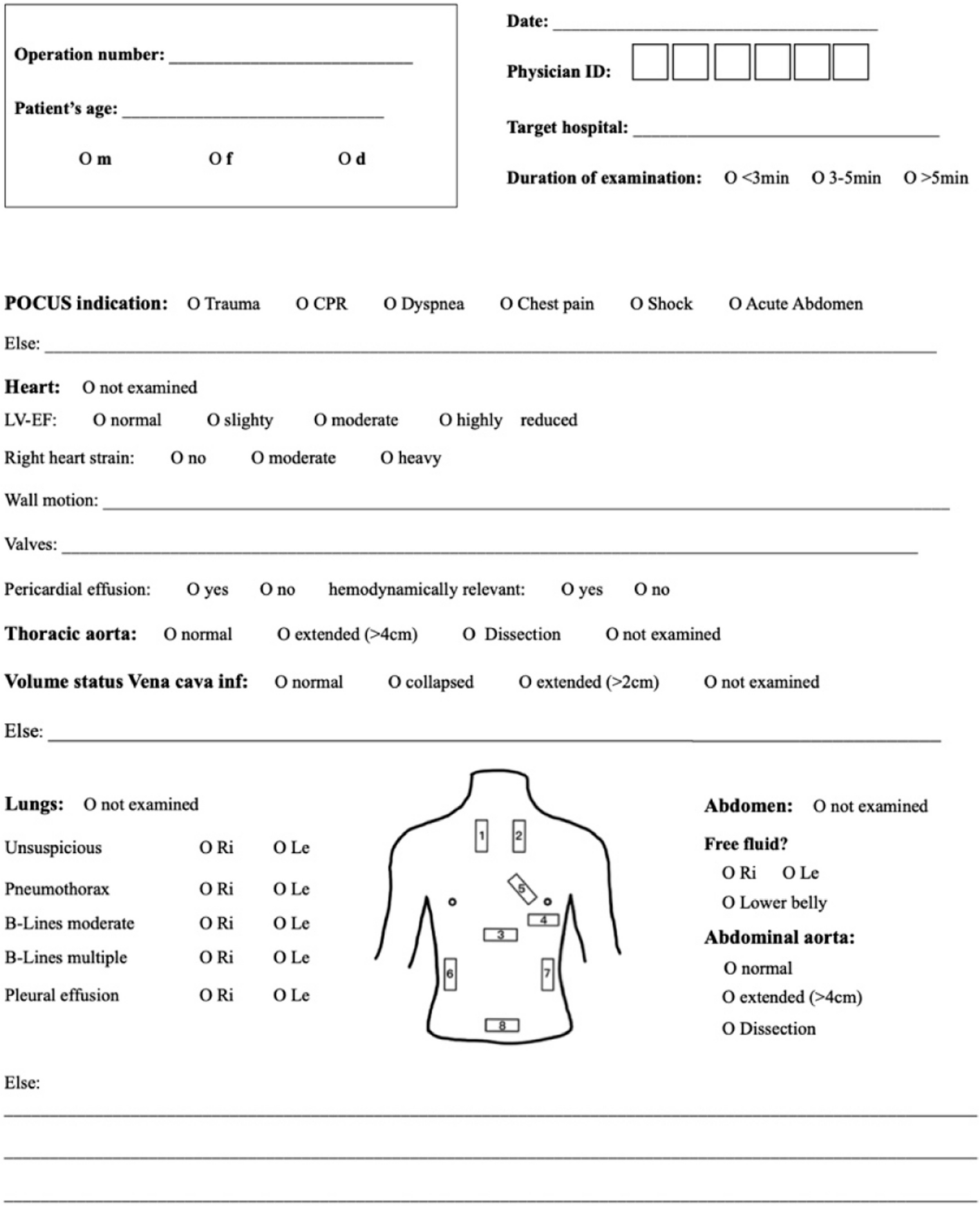
We also addressed the question of what intensity of POCUS training is needed for safe use in prehospital patient care. We found a high agree of agreement when comparing our cohort’s prehospital POCUS findings with in-hospital results (79.5% in total). A high level of safety was observed, particularly in the search for critical life-threatening pathologies such as pneumothorax (correctly diagnosed in 91.7% of cases), pericardial effusion (correct in 89.2%) or free abdominal fluid after trauma (86.9%). Even in examining the left ventricular function of the heart (LV-EF) which requires a higher level of expertise than e.g. the assessment of B-lines over the lungs, a high level of agreement between the findings was observed (correct in 60%).
In the vast majority of other prehospital POCUS publications, participants have had special training in POCUS examinations before or further education during data collection (2;3;5;6). Most EMS physicians in Germany are not necessarily well-trained and specialized in using ultrasound. We compared the prehospital ultrasound findings with the results of in-hospital radiological diagnostics during emergency department care. Participating EMS physicians were divided into different levels of competence in emergency ultrasound examinations using a developed scoring system.
Unfortunately, no statistically significant difference was found between groups with different levels of expertise.
This raises the question of whether, conversely, practical experience plays no role in the correct use of emergency ultrasound. The experience gained from the application and logic say no. What we found is that even EMS physicians with a low level of expertise in ultrasound examinations seem to be able to perform POCUS correctly at the prehospital scene. It must be taken into account that the number of examinations carried out by inexperienced emergency physicians was very low compared to the number of (very) experienced physicians and only a few examination results were documented for the respective findings. Findings were correct in a high number of cases and remain in good correlation with those obtained in-hospital. Of course, safe use requires training and regular practice. However, data suggests that one does not need to be a highly trained specialist in ultrasound diagnostics to perform prehospital POCUS savely. With attended training courses (like pPOCUS—prehospital Point of Care Ultrasound) and consistent use of ultrasound (e.g. several times/month), reliable findings for patient’s care can be obtained safely. It is essential to remember that competence and training in emergency POCUS are necessary. It is not sufficient to simply roll out mobile ultrasound devices area wide. Educational training concepts like pPOCUS, focusing prehospital ultrasound use are needed.
Limitations
When considering the results, several limitations must be taken into account. This study was a prospective observational trial. For obvious reasons no randomization or blinding was conducted. There were no guidelines for the participating EMS physicians regarding whether or which symptoms POCUS examinations should be performed prehospital. The decision was left to the respective EMS physician. The same applied to the documentation of the examinations. It cannot be ruled out that not all examinations were documented.
Follow up in-hospital data was available in only 108 cases. There was a high number of „lost cases “ due to no transport to a hospital or the inability to obtain the in-hospital findings. The four emergency ambulances in Nuremberg city complete around 23,000 missions per year (data from the rescue control center of the City of Nuremberg). Only a number of 258 POCUS examinations were documented as part of our study. Of the approximately 100 EMS physicians in the Nuremberg City ambulance service, only 32 participated in the study. Regarding this, a possibility of selection bias must be taken into account. Emergency POCUS was mostly performed by (very) experienced providers. There was just a small number of POCUS inexperienced EMS physicians. So we had limited data available for comparison between EMS physicians with different levels of competence.
Additionally, from a medical point of view, sonographic findings may already will change during prehospital treatment. The examination results in the ED may already be different, even though the ultrasound findings were correctly recorded prehospital. For example, the extent of heart failure may improve rapidly as a result of initial treatment, leading to an increased LV-EF over time, or no B-lines may be visualized over the lungs as treatment progresses.
The question of whether the study’s POCUS findings had an influence on prehospital treatment, therapeutical or organizational questions during prehospital care is part of an additional study, results are not discussed in this manuscript.


Comments (0)