
Remember me
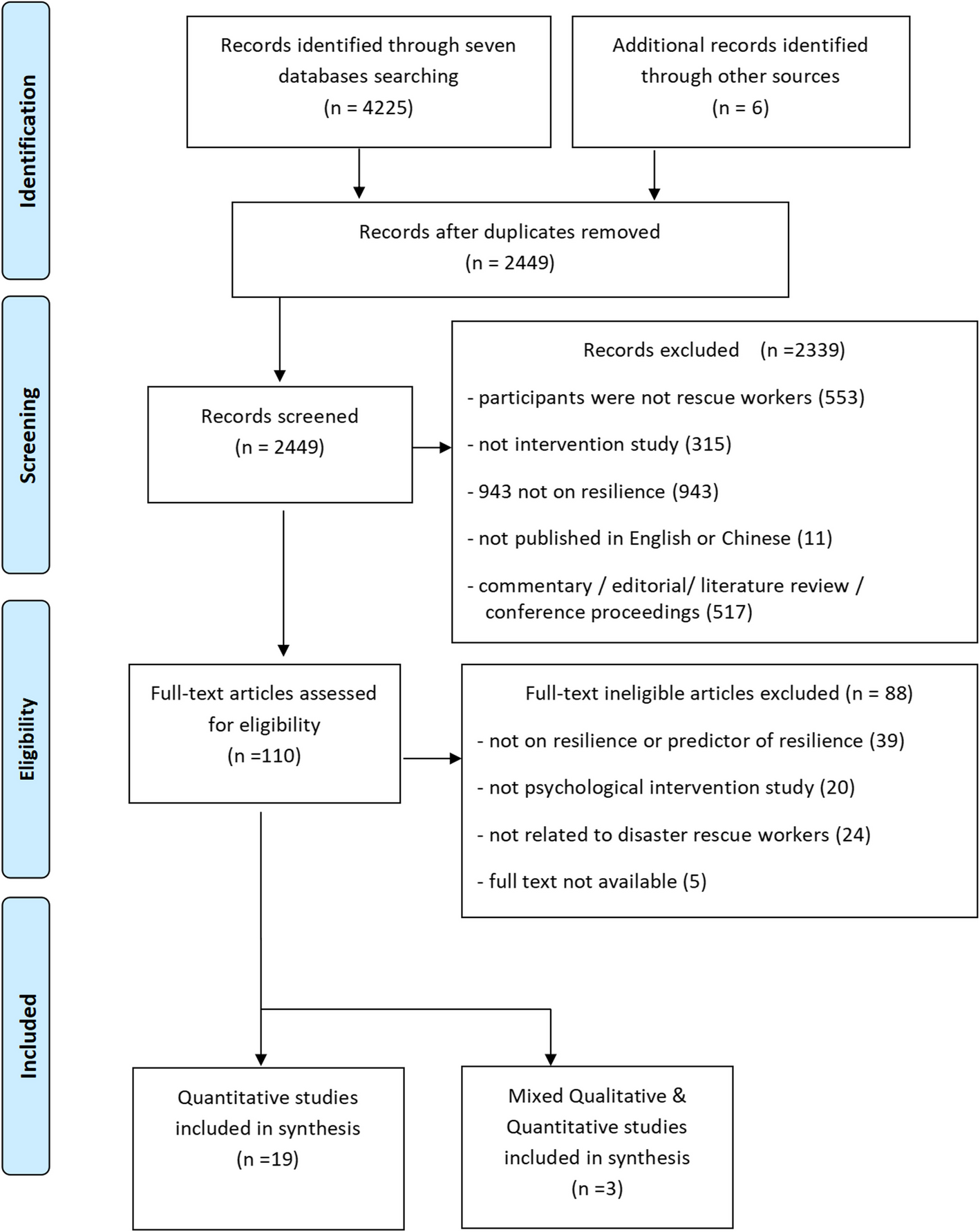

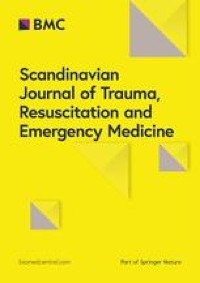
A total of 4231 citations were identified through the database search, and an additional six records were identified through other sources. After removing duplicates, 2449 articles were screened using titles and abstracts. A total of 4127 articles that did not meet the inclusion criteria were excluded. The remaining 110 full-text articles were assessed for eligibility. Finally, a total of 22 studies that met the inclusion criteria were included in this review. The process of selection for this review is outlined in Fig. 1.
Fig. 1
The process of literature search and selection
A total of 22 studies, consisting of 19 quantitative studies and three mixed-method studies were included in this review. Among the 19 included quantitative studies, six were randomized controlled trials (RCTs), and 13 were non-randomized studies (NRCTs). These intervention studies were published between the year of 2008 and 2024. The included studies were primarily conducted in Western countries, with the United States of America (n = 12), Australia (n = 2), England (n = 1), Netherlands (n = 1), and Canada (n = 2). Other studies were conducted in Egypt (n = 1), mainland China (n = 1), Iran (n = 1) and Taiwan (n = 1). The population of rescue workers included in these studies were military personnel/soldiers (n = 7), healthcare workers (n = 6), marines (n = 2), police officers (n = 3), firefighters (n = 2) and mixed personnel (n = 2) involved in disastrous events. The sample size of the 22 studies ranged from 21 to 12,529, involving a total of 24,227 rescue workers. The two studies'response rates only were 48% [7] and 69%, respectively[12], and the attrition rate of these studies ranged from 0% to 59.4%. The principal reasons given for dropping out of the interventions were due to the work schedule and military redeployment [7, 12, 50] or leaving the army due to being wounded or killed in combat [37].
Quality appraisal of included studiesThe results of the quality appraisal were presented in the last column of Table 1.
Table 1 summary of include studies characteristics and resultsAccording to the Mixed Methods Appraisal Tool (MMAT) criteria [14], while 20 out of 22 included studies obtained a quality score of 50% [5, 7, 9, 12, 13, 17, 19, 21, 23, 24, 29, 37, 42, 47, 49, 50, 55, 57, 59, 61], the other two were 25% [30, 32]. The quality of the 20 studies was fair, and two were relatively poor.
Twenty-two studies were included in this review, all meeting the inclusion criteria. However, several methodological limitations need to be highlighted. The randomized controlled trials [5, 13, 17, 19, 42, 57] did not report the randomization process or allocation concealment, which may introduce selection bias and affect the validity of the results. The non-randomized controlled trials exhibited various limitations, such as not recruiting participants in a manner that minimizes selection bias [37], failing to describe the appropriateness of measurements [12, 30, 32], lacking a control group [7, 9, 12, 23, 24, 30, 32, 47, 49], or not achieving an acceptable response rate of 60% or above [7, 37]. The mixed methods studies [9, 55, 59] did not explain the rationale for integrating qualitative and quantitative methods to answer the research question, which may limit the interpretability and coherence of the findings.
Characteristics of interventionsA summary of the characteristics of these interventions are outlined in Table 2.
Table 2 Summary of intervention characteristics of the included studiesThe interventions adopted approaches such as psychological education/support (n = 9) [9, 17, 19, 23, 32, 47, 50, 55, 57], mindfulness-based intervention (n = 5) [12, 24, 29, 30, 59], resilience training (n = 5) [7, 37, 42, 49, 61], cognitive-behavioral program (n = 2) [13, 21], and training of coping strategy (n = 1) [5]. Most interventions were delivered face-to-face in a group by psychologists (n = 11), resilience/mindfulness trained trainers (n = 4), army officers (n = 2), healthcare workers (n = 2), and social workers (n = 1). At the same time, the two studies did not mention the person who delivered the intervention [19, 24].
The interventions were delivered at various time points related to disaster deployment, some before deployment (n = 6), the majority during deployment (n = 12), and fewer after deployment (n = 4). There was considerable variation in the dosage and duration of these interventions. For the psychological education/support interventions, one study provided three consecutive days of 8-h psychological education sessions; another study offered an initial 2-h session followed by sessions ranging from 70 to 90 min for one month; two studies comprised sessions of 1 to 1.5 h each over a period of 4 to 8 weeks; four studies provided psychoeducation ranging from 2 to 10 h in total; one study did not report the dosage and duration of the intervention. The four mindfulness-based training studies were offered for two hours per session for 8 weeks, with an extended course of 4 to 8 h in the sixth or eighth week, while another online study lasted for 15 weeks with no dosage specified. For resilience training, two studies did not specify dosages but lasted for four sessions and 12 weeks, respectively; one study provided 8-h lectures for 10 days; another consisted of 2.5 h per session per week for 6 weeks; one offered courses lasting from 1.75 to 4.5 h with a flexible completion schedule. The one study that used a cognitive-behaviour approach consisted of two 40-min sessions for 6 weeks, while the dosage was not mentioned in another study. The one study of a coping training programme redundant consisted of 2 h each session per week for 14 weeks. The dosage and duration of these interventions are summarized in Table 2.
The effectiveness of interventions was measured immediately (n = 15), 1 month (n = 3), 3 months (n = 3), and 6 months (n = 1) after completion of interventions. Only ten of the 22 included studies reported follow-up assessments, with evaluation periods ranging from two weeks to 12 months after the intervention.
The most common intervention was didactic instruction (n = 16). Others were group discussion (n = 6), skills practice (n = 6), work assigned to do at home (n = 5), doing worksheets (n = 2), role-play (n = 2), and debriefing approach (n = 2). Three studies did not describe the format of their interventions [7, 23, 55].
Content of resilience enhancement interventionThe content of the interventions mainly included stress management [5, 19, 21, 23, 29, 30, 37, 42, 49, 55, 57, 59, 61], coping strategies [
Comments (0)