This study shows that follicular phosphate concentrations are positively correlated with serum phosphate, which suggests that follicular phosphate may be susceptible to dietary changes or therapies that regulate phosphate absorption, renal excretion, or mobilization from storage such as the skeleton. Despite the correlation with serum phosphate concentration, follicular phosphate concentration was significantly higher than serum concentration in women who did not achieve a live birth, while this was not the case for women who achieved a live birth. The lack of significance in the live birth group may be a chance finding due to the small sample size and should only be considered exploratory and warrants further investigation.
Although the absolute difference in follicular phosphate concentrations between serum and follicular fluid is modest (0.11 mmol/L), this finding may still hold biological significance. Systemic phosphate regulation is tightly maintained by hormones such as parathyroid hormone, FGF23, and active vitamin D [11], and even minor deviations can influence physiological processes. This difference may serve as a marker for increased cell turnover, as elevated follicular phosphate concentrations may be a result of the release of intracellular phosphate into the follicular fluid. Intracellular inorganic phosphate concentrations do not diverge significantly from those in serum, with values generally ranging from 0.7 to over 2.0 mmol/L [19]. However, a large fraction of phosphate intracellularly is available as organic phosphate that also can be released and may contribute to the higher phosphate content during cell lysis. To the best of our knowledge, follicular phosphate concentrations have not previously been reported in humans, although studies in animal models have shown comparable phosphate concentrations in serum and follicular fluid [20].
The precise mechanisms governing the transport of minerals such as phosphate across granulosa cells into the follicular fluid are not yet fully understood. A clinical study with tritium-labeled injections revealed the presence of tritium in follicular fluid an hour post injection, suggesting that follicular fluid composition is influenced by serum composition [21]. Nevertheless, our results could imply an active transport process of phosphate into the follicle with a tightly regulated phosphate environment in the follicular fluid. This aligns with the current understanding that follicular fluid is a complex mixture of serum-derived components and locally synthesized factors within granulosa cells [22]. If phosphate is actively transported into the follicle, low serum phosphate concentrations could lead to correspondingly low phosphate concentrations in follicular fluid due to limited availability (Fig. 2A). In the absence of direct evidence from our study, these interpretations remain hypothetical, underscoring the need for future mechanistic investigations to elucidate the pathways of phosphate regulation in the follicular environment. The moderate correlation between follicular and serum phosphate (r = 0.43, p = 0.007) suggests that while systemic influences are evident, local regulatory mechanisms within the follicular microenvironment may also be important. Although analogous examples in the female reproductive tract are limited, observations from other systems—such as the precise control seen in renal and skeletal mineral homeostasis—underscore that small differences in mineral concentrations can have significant biological impacts. Further research is warranted to delineate the relative contributions of systemic versus local regulation on follicular phosphate levels.
In this study, we identified a positive correlation between phosphate and testosterone in follicular fluid, contrasting with a trend toward a negative correlation in serum. The correlation between phosphate and testosterone in follicular fluid might be influenced by the stimulation protocols applied during ARTs. Some women are treated only with FSH while others are treated with both luteinizing hormone/human chorionic gonadotropin (hCG) combined with FSH, which have different stimulatory effects on the follicle. While the serum correlation did not reach statistical significance – likely due to the small sample size – the lack of correlation between serum and follicular fluid testosterone concentrations has been observed previously by a study on women in natural menstrual cycles which also found no association between serum and follicular fluid testosterone [23]. Studies have previously demonstrated age-related declines in serum testosterone and lower testosterone concentrations associated with a reduced number of secondary follicles [4, 24, 25]. We did not find this correlation, possibly, as our cohort had a quite narrow age range. Furthermore, the observed positive correlation between follicular phosphate and testosterone may be mechanistically linked to the role of phosphate in cellular energy metabolism. Phosphate is essential for ATP production, a key driver of the energy-demanding process of steroidogenesis in the ovarian follicle. Enhanced ATP production could facilitate increased steroidogenic activity in theca cells, thereby elevating local testosterone synthesis. Nonetheless, as no previous studies have directly investigated this relationship in follicular fluid, these interpretations remain speculative. Future mechanistic studies are needed to elucidate whether phosphate directly influences testosterone production through metabolic pathways in the follicular microenvironment.
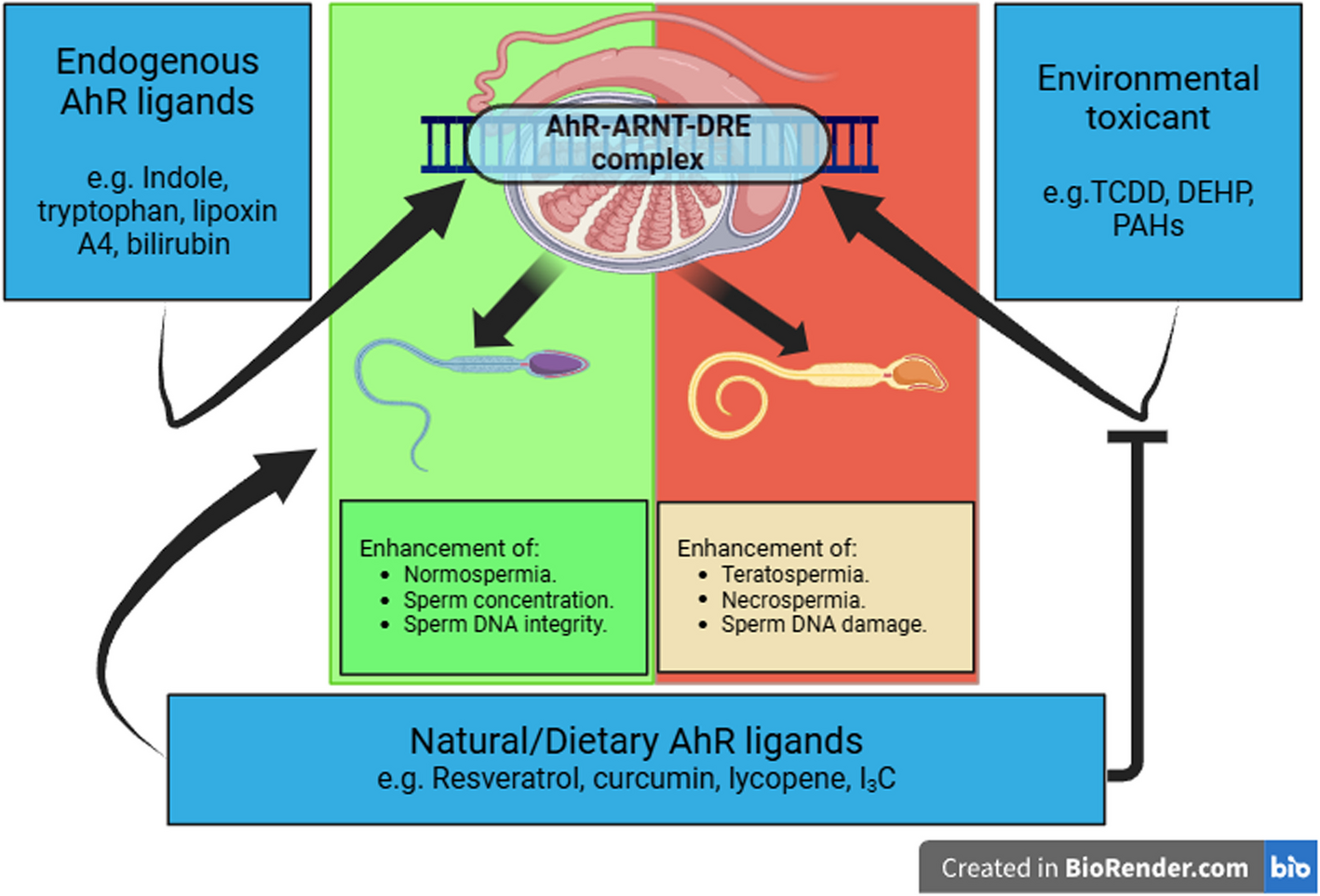
The trend towards a possibly favorable high-concentration phosphate and low-concentration calcium in the follicle seems to be the opposite in the male reproductive tract. In male reproductive health, the role of phosphate is not completely understood although recent data suggests a role in both testicular and epididymal function [26, 27]. Remarkably, seminal fluid contains phosphate at concentrations several fold higher than in serum [14]. Semen quality has been shown to be negatively influenced by reduced seminal fluid concentration of both calcium and phosphate [28, 29], while the presence of phosphate and calcium during in vitro fertilization may increase the competence and efficiency of the sperm [30]. This divergence may be attributed to fundamental differences in the physiological roles and regulatory mechanisms governing mineral homeostasis in the female and male reproductive systems, which are likely tailored to support the distinct requirements of oogenesis and spermatogenesis, respectively. Therefore, the role of the minerals in the reproductive tract is complex, and whether phosphate can play a role in oocyte quality in the female reproductive tract needs to be explored.
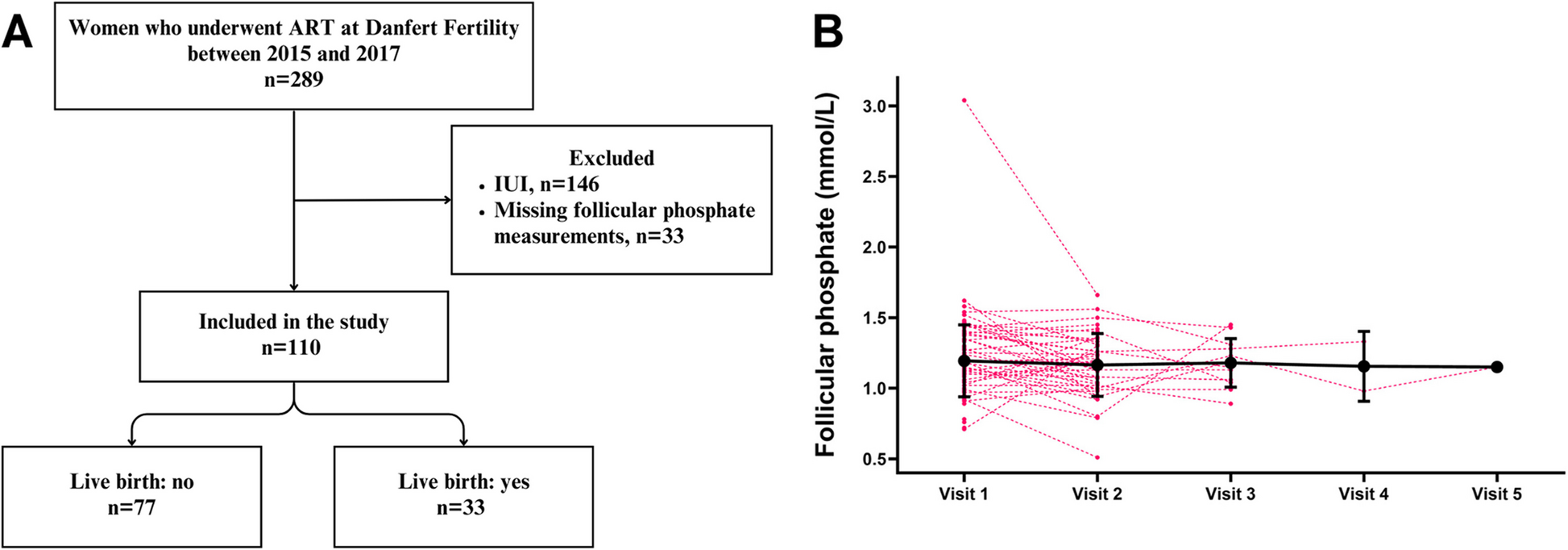
Our study's primary strength is the novelty of measuring phosphate in follicular fluid together with other minerals and hormones. However, some limitations exist for instance the pooling of follicular fluid into a single composite sample per cycle per participant; thus, this may mask important variations between individual follicles. Future studies could benefit from analyzing individual follicular fluid samples to identify biomarkers or mechanisms linked to oocyte quality, which may be obscured in pooled analyses. This could enhance personalized fertility treatments and improve ART outcomes. Additionally, variability in the timing of serum sample collection presents a limitation; samples were obtained either on the day of oocyte aspiration or up to two weeks earlier. This variability may explain the difference in follicular fluid and serum concentrations of measured minerals. Despite these constraints, the use of mixed linear regression models demonstrated significant stability in mineral measurements over time for the same individual, and strong correlations between compartments support the robustness of our findings. Clinical data for participants were extracted from routine patient records, reflecting the standard workflow in a private fertility clinic. Stratifying participants by conditions such as polycystic ovarian syndrome, rather than focusing solely on ovulatory status, could provide greater clarity in regard to the regulatory mechanisms of minerals. This study is limited by the relatively small number of live births and the subset of participants with paired serum samples, both of which may reduce statistical power and introduce potential selection bias. Consequently, some findings should be interpreted with caution, as Type II errors cannot be ruled out. Future studies with larger, well-powered cohorts and more comprehensive sampling are needed to validate these observations. Due to the exploratory nature of this study, no formal corrections for multiple testing were applied. Therefore, the results should be interpreted with caution, considering the increased risk of type I errors. Future studies may benefit from a design with sufficient power to demonstrate clinical significance, ideally through a randomized controlled trial (RCT). Potential confounding factors, such as dietary phosphate intake, vitamin D status, FGF23, parathyroid hormone levels, or ICSI treatment were not accounted for in our study. These variables could significantly impact both systemic and follicular phosphate levels and should be considered in future research to determine the clinical relevance of our findings more accurately.
In conclusion, our findings suggest that follicular phosphate levels are influenced by systemic phosphate homeostasis, but their role in ART outcomes remains unclear. Future studies with larger sample sizes and mechanistic investigations are required to determine potential clinical relevance.





Comments (0)