In this study, we demonstrated comparable euploidy rates of blastocysts in PGT-A cycles between the PPOS protocol and the GnRH antagonist protocol. Euploidy rates remain similar across different age subgroups within these two groups. Furthermore, pregnancy outcomes, including clinical pregnancy rate and live birth rate in FET cycles, were identical. However, the miscarriage rate in the PPOS group was lower than that in the GnRH antagonist group.
Several studies about PPOS have been conducted to investigate its administration and efficacy [4, 6]. First, the vast majority of prospective and retrospective IVF/ICSI studies [13,14,15,16,17,18] demonstrated no differences in retrieved outcomes between PPOS and GnRH antagonist protocols, including the number of oocytes, MII oocytes, fertilization rate, morphological score of D2-3 embryo, and viable blastocysts. However, a retrospective study including 1652 PGT-A cycles of social fertility preservation reported by Giles et al. [8] found that more oocytes were retrieved in PPOS protocol, while other retrieved outcomes were equivalent to those in GnRH antagonist protocol. The increased retrieved oocytes may be due to a higher total gonadotrophin dose in PPOS [8]. In another small sample retrospective cohort PGT-A study, a higher MII rate and fertilization rate, along with a lower blastocyst rate, were detected in the PPOS group, but the number of oocytes retrieved was similar between PPOS and GnRH antagonist groups [7]. In our study, we found an identical number of blastocysts but fewer oocytes, MII oocytes, two pronuclei zygotes, and D3 good-quality embryos in the PPOS group compared to the GnRH antagonist group. However, it should be noted that this difference might be resulted from lower AMH levels and higher baseline FSH levels in PPOS, although the difference was not significant. A higher initial gonadotrophin dose also suggested more women with decreased ovarian reserve in PPOS. A randomized controlled trial may be necessary, as the retrieved outcomes among these retrospective studies in PGT-A cycle were inconsistent.
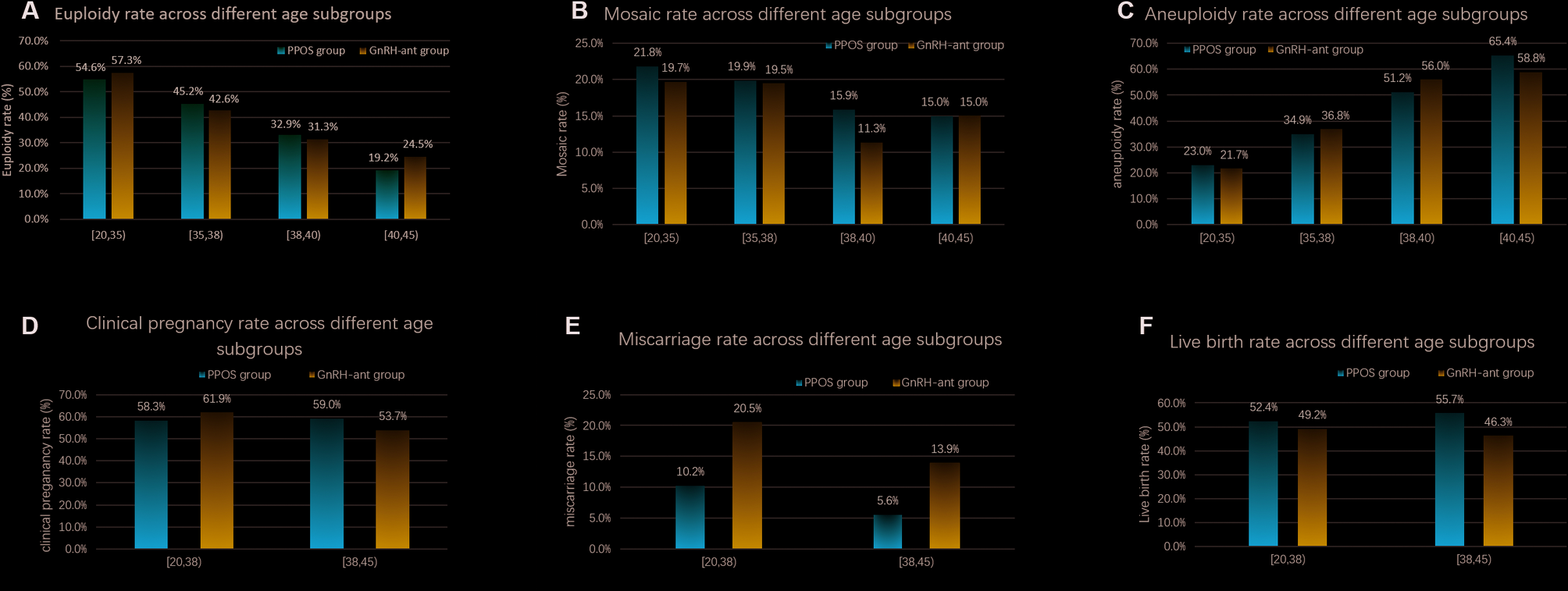
Second, several studies have retrospectively compared euploid blastocyst rates between PPOS protocol and GnRH analog protocols [7,8,9,10, 19,20,21]. According to a recent retrospective cohort study, oocytes retrieved, MII oocytes, fertilized oocytes, and viable embryos were comparable between dydrogesterone and MPA when PPOS was applied in women with polycystic ovarian syndrome [22]. However, the euploid blastocyst rate between MPA and dydrogesterone remains unclear. In these studies using MPA, the euploid blastocyst rate was from 31.8 to 38.7% [7, 8, 19]. Our study showed a slightly higher euploidy rate of 43.3% when MPA was used in the PPOS protocol, which may be attributed to the younger female age in our study. In these studies using dydrogesterone in PPOS, two studies protocol showed similar euploidy rates of 34.88% [9] and 33.14% [21], while a higher euploidy rate of 46.5% was noted in Wang et al.’s study [20]. Above all, most studies showed a similar blastocyst euploidy rate between deydrogesterone and MPA.
On the other hand, the euploidy rate per biopsied blastocyst were comparable between PPOS and GnRH antagonist according to previous studies [8, 9, 19,20,21] and our study. In different age subgroups of PPOS and GnRH antagonist, both Yang et al.’s study [9] and our study showed no significant difference in euploidy rate. However, Pai et al. reported a lower euploidy rate in the elder subgroup (≥ 38-year-old) of the PPOS group [7]. The significant result from Pai et al.’s study [7] should be interpreted with caution, as only 19 PPOS cycles were enrolled in the elder subgroup. Wan et al. found a higher euploidy rate in women aged ≥ 35 years undergoing the PPOS protocol [10]. Additionally, the aneuploidy rate per biopsied blastocyst was lower in PPOS than in GnRH antagonist although the euploidy rate were similar according to the study by Giles et al. [8]. In this study by Giles et al., it should be noted that women in the ≤ 35 years subgroup undergoing PPOS protocol had a younger age than those with the GnRH antagonist protocol. In molecular testing, Oktem et al. found that exposure of antral follicles to MPA did not have any detrimental effects on steroidogenic, ovulatory, and luteal functions compared to GnRH antagonist cycles by analyzing luteinized mural granulosa cells [23]. Therefore, more good-quality studies are needed to confirm this question in the future, as all these studies were retrospective investigations.
Finally, pregnancy outcome is another indication for evaluating embryo quality from PPOS protocols. In the conventional IVF/ICSI, clinical pregnancy rates, miscarriage rates, and live birth or ongoing pregnancy rates were similar between PPOS and GnRH analogs according to a recent meta-analysis [24, 25]. Even in the women with decreased ovarian reserve or predicted suboptimal responders, MPA was considered a patient-friendly alternative to antagonists, as similar ovarian response and live birth rates were observed between the two groups [26, 27]. In this study, either clinical pregnancy rate or live birth rate was comparable in the PPOS group and GnRH antagonist group, which was consistent with previous studies in PGT-A groups [7,8,9, 19,20,21]. However, the miscarriage rate was lower in the PPOS group than GnRH antagonist group in both a large retrospective study by Giles et al. [8] and our study. In another two small sample studies [7, 20], the miscarriage rate was also higher in the GnRH antagonist group than the PPOS group, although the difference was not significant. Therefore, the PPOS protocol seemed to yield a lower miscarriage rate than the GnRH antagonist protocol, as the clinical pregnancy rate and live birth rate were similar between these two protocols. A prospective randomized controlled study may be necessary to confirm this issue since all these studies were retrospective and the causes of miscarriage are highly complex.
Some limitations should be noted in the present study. First, this study was retrospective, non-randomized design. Although PSM and regression analysis were utilized to migrate bias from confounding factors, it may still influence the results. Some results from regression analysis should be interpreted with caution due to a low R2 value. Second, the generalizability of this study should be approached with caution, as it was conducted at a single center. Additionally, the limitation from PGT-A testing method should be noted, particularly regarding mosaicism, even though the cut-off (30% ~ 70%) was applied in this study. Finally, the sample size was small, particularly since they were divided into different subgroups. Overall, it is crucial to further validate these results through multicenter prospective randomized controlled studies with a large sample size.
In conclusion, our finding provided further evidence that PPOS protocol seems to be an effective option for couples undergoing PGT-A, as the genetic status of biopsied blastocyst and main clinical pregnancy outcome did not change in patients with PPOS protocol. Additionally, a lower miscarriage rate in these patients should be noted as another potential advantage, although this needs to be confirmed by further studies.





Comments (0)