Aim of the study, design, and setting
The aim of this study was to retrospectively evaluate the impact of early (< 6 months) versus standard (> 6 months) return to play (RTP) protocols on the rate of failure, volume of play, and career longevity following ACLR in a cohort of professional European soccer players. It was hypothesized that athletes returning to professional competition earlier than 6 months after ACLR would have an increased risk of failure, lower volume of play, and would play for fewer seasons following surgical intervention compared with those returning after 6 months.
Professional soccer players treated with primary anterior cruciate ligament reconstruction by a single surgeon (P.P.M.) between April 2008 and December 2016 were included in this retrospective study. The study was approved by the institutional review board (prot. Professionisti_OSS_22), and all study patients signed a consent form following written and oral information for the management of clinical data for research purposes. Eligible patients were treated at the study center from April 2008 to December 2016, with continued data regarding the patients’ ACLR failure and professional soccer status recorded through April 2023.
Study population
The inclusion criteria were that the patient was (1) male and a (2) professional soccer player undergoing a (3) primary anterior cruciate ligament reconstruction. The exclusion criteria were (1) ipsilateral prior ACL or ligamentous knee injury, (2) previous injury requiring surgery on the same limb, including fractures. The cohort was then divided into two groups on the basis of the time to RTP, defined as the time of the first match participation after surgery: the “Early RTP” group for those players returning to a match before 180 days from surgery and “Standard RTP” group for those returning after 180 days. The postoperative physical therapy accelerated protocol was the same for all the patients.
Data extraction and management
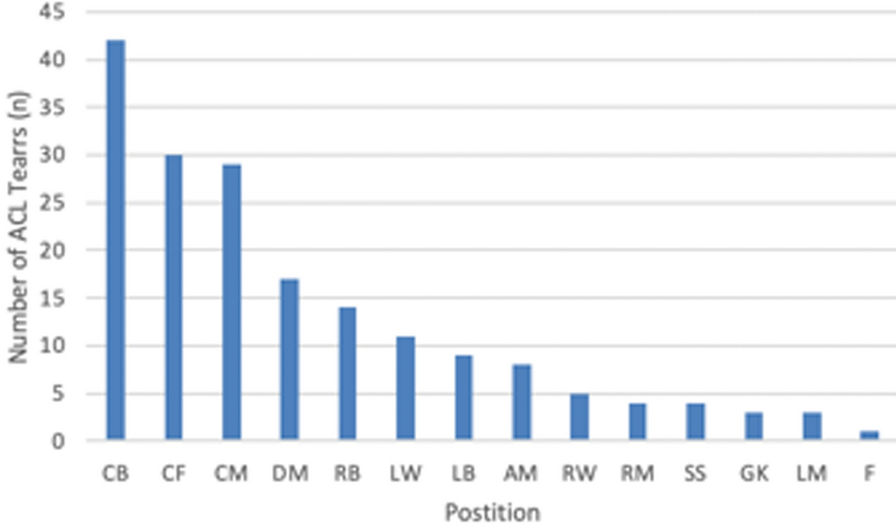
The patients’ position was recorded and categorized into (1) goalkeeper, (2) defensive player (e.g., center back, full back), (3) midfielder, and (4) attacker (e.g., forward, winger). The player’s club and league level at the time of injury were recorded.
Surgical technique
All patients were treated surgically with arthroscopic evaluation prior to autograft harvest. No allograft was used as it is not readily and safely available in Europe. The preference was for ipsilateral bone-patellar tendon-bone autograft. A notchplasty was performed in all cases to allow for proper positioning of the femoral tunnel through a tibial tunnel at the 10 o’clock position for right knee or 2 o’clock for left knee. Suspensory fixation was utilized for the femoral side and an interference screw (bioabsorbable) for the tibial side. Meniscal pathology, including root tears, were treated preferentially with a repair.
Rehabilitation protocol
All patients were admitted to the hospital overnight and began physical therapy postoperatively on day one. Patients were followed at the physiotherapy center for a minimum of 4 weeks after surgery prior to returning to their team physician, who supervised therapy and ultimately determined when the patients were permitted to return to play. For the first 4 weeks, the subjects worn a knee brace locked in full extension for the first 2 weeks and then locked 0–90°. Full weight bearing was allowed, unless a medial meniscal suture at the posterior horn (not including ramp lesions) or suture of bucket handle tears of the lateral meniscus. Exercises consisted in progressive resistance isometric strengthening for quadricep and flexor muscles, bike with progressive resistance, and stretching, with the progressive recovery of full ROM. Once the players returned to their team physician, rehabilitation protocol was not standardized but was in charge to the team physiotherapy staff. The treating surgeon was not involved in the rehabilitation program once the patient returned to their respective team physician, nor was the treating surgeon involved in the decision for timing of return to play. However, some key requirements must be met before the athlete was cleared for field rehabilitation by the surgeon: 20% limb symmetry index (LSI) for isometric maximal voluntary contraction of the quadricep, 10% LSI for countermovement jump peak ground reaction force, and 10% LSI for triple hop test. Ultimately, the respective team physician was responsible for the rehabilitation and return to play criteria for each patient.
Time from intervention to return to the first official game was recorded in days. Information if the patient returned in the same season was recorded, as well as the number of games and total and average minutes played in the return season. The number of seasons played after injury and if the player was active at the time of data collection (September 2019) were also recorded. Failure of ACLR, defined as a reinjury to the reconstructed ACL that required revision surgery, was also recorded.
Statistical analysis
Normality of continuous data was tested by visual inspection of histograms, QQ-plots, and the Shapiro–Wilk test. Continuous data were described with mean and standard deviation (SD), and median, range, frequency, and percentage were used for categorical data. Differences between groups were analyzed with the chi-squared test for categorical data and with Student’s t-test or the Mann–Whitney U test for continuous data. The statistical software, R, version 4.0.2, was used for all plots and analyses (access date 22 June 2020; R Core Team, Vienna, Austria, with the additional package ggplot2). The level of significant difference was set at 0.05.







Comments (0)