TBS is an index derived from the grey scale variation in a two-dimensional projection obtained by DXA of the spine and allows an estimation of fracture risk based on the indirect assessment of bone microarchitecture [12]. The clinical contexts in which TBS can be useful are manifold and for this reason, several studies have been carried out concerning its use. Since 2012, TBS has been studied in the management of patients with primary hyperparathyroidism, however, more than 10 years have passed and the clinical utility of TBS in the decision-making process for parathyroid surgery still remains uncertain.
For the aforementioned reasons, our study aimed to better characterize bone quality in PHPT patients, as also stated in the research agenda of the latest international guidelines [16], and to clarify the usefulness of TBS in clinical practice, proposing it as a means for identifying a proportion of PHPT patients at high fracture risk who could benefit from parathyroidectomy and may not be captured by other clinical tools.
Analyzing the characteristics of the study population, it emerged that patients with degraded TBS had lower T-score values at all sites than patients with TBS > 1.2, thus underlining the concordance of TBS and DXA in identifying patients with a high fracture risk. Furthermore, in our study 68.8% of patients presented degraded or partially degraded TBS, while only 36.8% showed osteoporosis at any of the 3 sites. This evidence is in line with literature, as in the study by Muñoz-Torres et al. [17], in which 72 patients with PHPT were enrolled, 51.4% presented a degraded TBS (in this study degraded TBS was considered as ≤ 1.23) and 73.6% had a TBS < 1.31. Of these 72 patients, only 37.5% were osteoporotic according to the BMD values of the three sites. The study by Grigorie et al. [18] also agrees with our study, as out of 153 patients with PHPT 32% presented degraded TBS, 51% partially degraded and 17% preserved. This evidence suggests that TBS is able to detect a greater proportion of patients with an increased risk of fracture than BMD alone, precisely because of its ability to identify the qualitative degradation of bone microarchitecture. It should also be noted that 17 patients in our study had been taking oral bisphosphonates for less than two years (mean duration of therapy was 387 days). This did not impact BMD classification of the patients compared to the starting point of these medications (i.e. the diagnosis of osteopenia or osteoporosis remained stable).
Classifying patients according to lumbar spine BMD categories, osteoporotic patients showed lower TBS values compared to both osteopenic patients and to those with normal BMD. This finding is in partial agreement with the study by Munoz-Torres et al. [17], in which TBS values were lower in osteoporotic patients compared to normal BMD (1.16 ± 0.12 vs. 1.26 ± 0.17; p =.043), but not to osteopenia.
Analyzing the cohort of patients with osteoporosis at the third distal radius, a strong association was seen with low TBS (p =.003). The group of patients with TBS ≤ 1.2 had an almost two-fold greater incidence of osteoporosis at the distal third of the radius than patients with TBS > 1.2. This association supports a pathophysiological role of PTH excess both on cortical bone and trabecular bone. In any case, forearm DXA still remains essential in the management of PHPT patients because, as demonstrated by Castellano et al. [19], this assessment also increases the rate of patients with asymptomatic primary hyperparathyroidism meeting surgical criteria.
Another debated issue is the association between TBS and biochemical indices in patients with PHPT. There is conflicting data in the literature, with two studies [20, 21] showing that there were no associations between TBS and various biochemical indices. Two other studies contrasted this evidence, the first [22] showing an association between TBS and BAP values, and the second [23] showing an association between TBS and 25(OH)D values. In our study, there were no significant differences in biochemical indices between patients with degraded and not degraded TBS. In particular, after adjusting for age and BMI, no differences were noted in eGFR and urinary calcium values because as expected degraded TBS is more frequent in older patients who often show declined kidney function and consequently reduction of urinary calcium excretion due to aging and/or or concomitant known disease involving kidney function (e.g. obesity and arterial hypertension).
Considering the distribution of patients with degraded TBS in the various surgical indications, the most relevant evidence is the higher incidence of fragility fractures or morphometrical vertebral fractures in patients with degraded TBS compared to those with TBS > 1.2. In literature, many studies confirm this finding, such as the one conducted by Romagnoli et al. [24] or the one by Eller-Vainicher et al. [25]. TBS’s ability to identify patients at increased risk of vertebral fractures is well established and it has been demonstrated in patients with PHPT [26, 27] as well as in patients with post-menopausal osteoporosis [28, 29].
Within osteopenic patients the percentage of those with degraded TBS was significantly lower than that in osteoporotic patients. Reasoning on the basis of the current Italian [30] and international [16] guidelines, however, it is very important not to underestimate this proportion of osteopenic patients with degraded TBS, because they still have significant fracture risk but may not meet surgical criteria, unlike their counterparts with osteoporosis. This evidence is also supported by the Manitoba study [31] carried out in Canada in 2011, which stated that the risk of fracture in post-menopausal women with osteopenic BMD and degraded TBS is equal to or greater than that of women with osteoporosis.
We found that within the cohort of patients who did not meet the current surgical recommendations (N = 13), (N = 3) 23.1% presented a degraded TBS, and these patients had osteopenia. Thanks to this last piece of evidence, we understand the added value of performing TBS in clinical practice; in fact, by implementing its use in the clinical routine, we could identify a substantial proportion of patients with degraded TBS and osteopenia who would not otherwise be referred to surgery, but who nevertheless carry an increased fracture risk.
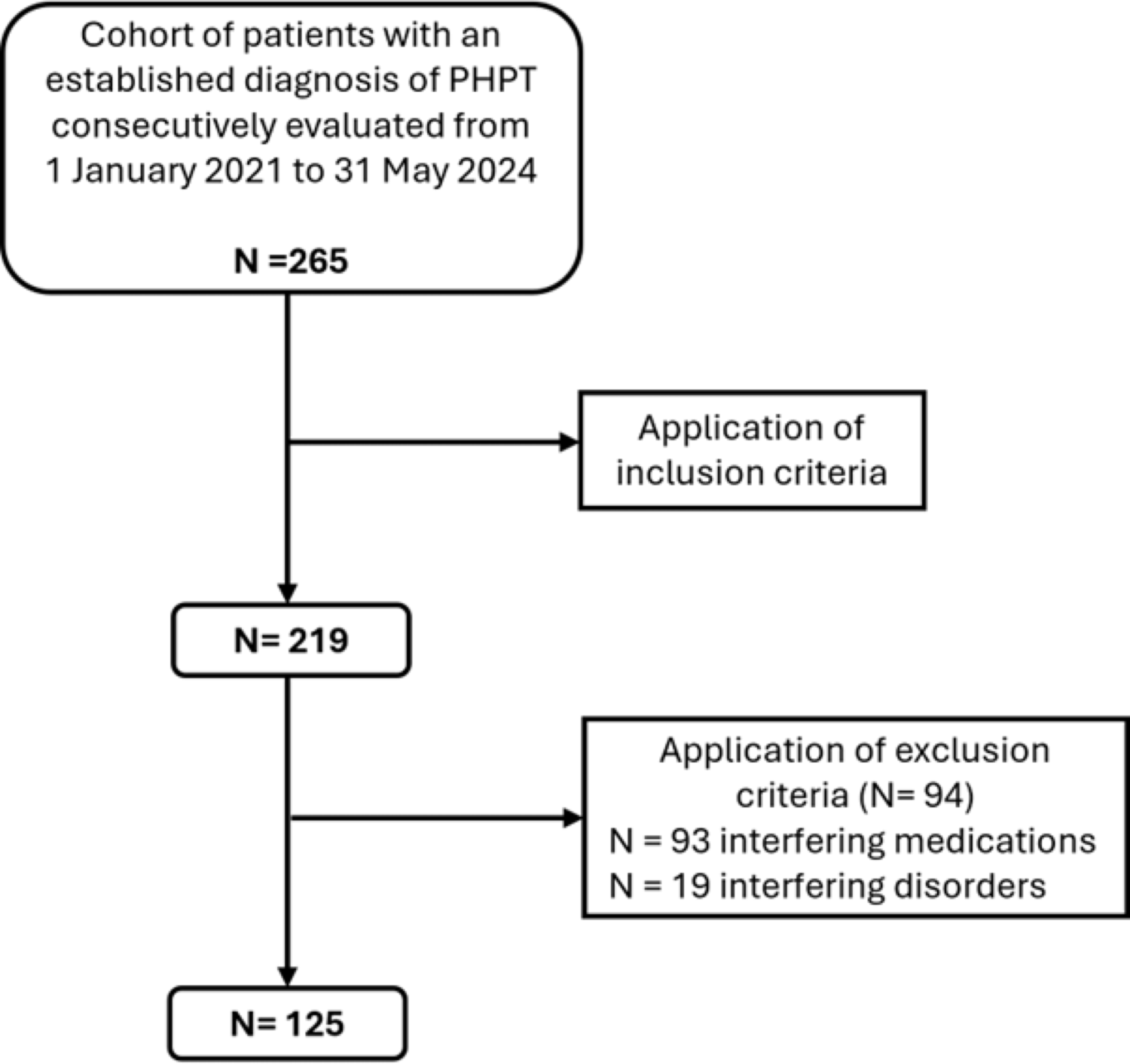
The strengths of this study were the single-center design and the exclusion of most drugs and disorders interfering with calcium-phosphorus metabolism or with bone quality. Also, all patients had a DXA performed with TBS at the 3 recommended sites (lumbar, hip, radius) with the same DXA machine, and underwent complete serum and urinary assessment in the same laboratory. The limitation of this study is the retrospective design as residual confounding might be present, as well as the cross-sectional analysis, as no follow-up information was provided to inform on the predictive power of TBS in the risk of incident fractures in PHPT. We also acknowledge a relatively small number of patients to draw definitive conclusions on the precise proportion of patients with degraded TBS alone and with no other surgical criteria. This last figure might be dependent on the study population examined.


Comments (0)