
Remember me


Akhverdyan Y, et al. Annal Rheum Dis 2017;76:1149
2.Papichev EV, et al. Osteoporos Int 2019;30:S.381
3.Polyakova J, et al. Annal Rheum Dis 2019:30:S.387
P122 Right care, first time: osteoarthritis, mental health, and sleep disturbancesC. Walker1, A. Bajaj 2 1Viatris, Hatfield, UK, 2Viatris, Bengaluru, IndiaMultiple studies demonstrate that 20–25% of osteoarthritis (OA) patients experience affective disorders including depression or anxiety however the impact of comorbid depression on the treatment of OA has not been as well evaluated. OA also commonly associates with significant sleep disturbances, particularly in the elderly and negative bidirectional effects of pain on depression and sleep disturbances are potentially overlooked.
Chronic pain and mental health: OA is associated with persistent and chronic pain as a primary symptom of the disease. Multiple studies have shown that chronic pain depicts a fundamental risk factor for the development of depression and disturbances in sleep. Being female, higher baseline WOMAC pain and dysfunction score and having two or more painful sites, increase the risk of depression. Ageing is a risk factor for OA, but not a risk factor for depression, with ageing also reportedly being linked to an increased likelihood of poorer sleep (both quantity and quality). Systematic reviews have revealed that OA patients diagnosed with anxiety and/or depression experienced more pain, had frequent hospital visits, took more medication, and reported less optimal outcomes. Also, depression and anxiety were found to be predictors of complications after primary total joint arthroplasty and have been associated with higher healthcare costs, extended length of hospital stay, or increased postoperative mortality after TKA/THA (Total Knee/Hip Arthroplasty).
What can we do? Depression may serve as a better predictor of disability than radiographic degenerative joint changes and indicate amplified pain and functional disability. Routine psychological screening could be beneficial for OA patients. Early diagnosis, counselling on mood and sleep hygiene, psychological support, exercise, antidepressant pharmacotherapy and/or problem-solving treatment and interdisciplinary collaboration should be a part of the core management strategy in OA patients.
Conclusion: Depression and sleep disturbances increase the health-related burden of OA. Greater attention to these comorbidities and overall health among patients with OA is warranted. Detecting and managing mental health issues, and chronic sleep disturbances could pave the way for better management of OA.
P123 Artificial intelligence in musculoskeletal health: the what, how and why? A. Bajaj 1, C. Walker2, R. Chiaese3, S. Er4 1Viatris, Bengaluru, India, 2Viatris, Hatfield, UK, 3Viatris, Monza, Italy, 4Viatris, Istanbul, TurkeyUse of artificial intelligence (AI), and machine learning (ML) has increased in numerous critical medical sectors, significantly impacting patients' and practitioners’ lives. AI-aided systems are increasingly available for diagnosis, management and physiotherapy rehabilitation in musculoskeletal conditions providing benefits to the patient and efficiencies for healthcare systems.
Applications of AI in Musculoskeletal Health: AI helps monitor and track pain triggers and assists patients and healthcare professionals in the identification of the most effective coping mechanisms. Mobile apps rather than manual approaches have been found to be more useful by patients to track joint pain, stiffness and buckling of knees potentially assisting in early diagnosis. New AI-enabled tools can also monitor patient's mental health and warning signs by capturing brief voice samples and analyzing them for signs of depression or anxiety. Therapists accessing data from AI apps can easily and remotely monitor patients' conditions. AI can also be helpful in orthopaedic surgeries to help decide whether to perform surgery, preoperatively estimate the risk of complications or mortality, the functioning of the prosthesis, as well as predict the duration of hospital stay, with accuracy and reliability.
Limitations of AI: To maximize the usefulness of AI the quality of data must be safeguarded, and the quantity of data maximized to avoid drawing erroneous conclusions. Additionally, AI can't reliably provide a causality assessment for chronic painful conditions.
Conclusion: AI systems that are practical, solution-driven, cost-effective, and easily accessible are the goal for large patient populations. Cutting-edge AI-imaging and ML technologies are potentially beneficial in lowering pain and enhancing functional impairment in patients with musculoskeletal diseases. The use of some technologies may be challenging in older age groups but is not insurmountable when help is provided.
P124 Correlation between DXA and HR-PQCT in osteogenesis imperfecta: preliminary findings in a cohort of adult patientsS. Gazzotti1, R. Sassi1, E. Schileo2, G. Fraterrigo2, A. Moroni3, M. Miceli1, M. P. Aparisi Goméz4, F. Taddei2, L. Sangiorgi3, A. Bazzocchi 1 1Diagnostic and Interventional Radiology, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy, 2Bioengineering and Computing Laboratory, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy, 3Dept. of Medical Genetics and Rare Orthopaedic Diseases, and CLIBI Laboratory, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy, 4Dept. of Radiology, Auckland City Hospital, New ZealandObjective: To evaluate the correlation between areal BMD (aBMD) measured by DXA and HR-pQCT parameters in adults with osteogenesis imperfecta (OI).
Methods: The present report includes preliminary data from 14 adult patients (mean age: 36 y) with OI enrolled in an ongoing prospective study. aBMD was measured with DXA (Hologic QDR Discovery Wi) at the lumbar spine, hip, forearm (1/3 and ultradistal radius), and total body. HR-pQCT (XtremeCT II, SCANCO Medical), a noninvasive modality that couples high resolution and low dose in vivo to gain insight into bone microarchitecture, was performed at the distal radius and tibia using a fixed offset protocol and automatic contouring with standard XtremeCT II evaluation. A p-value < 0.05 was considered significant.
Results: DXA classified 4 out of 14 patients included in our cohort as having normal BMD. However, HR-pQCT revealed widespread deteriorations in most parameters of density and microstructure, enabling the identification of different bone phenotypes, despite the relative clinical homogeneity of the sample population. Total volumetric BMD measured by HR-pQCT at the distal radius correlated well with DXA-aBMD at the ultradistal radius (r = 0.75; p = 0.002) and this relationship predominantly reflected agreement in the cortical rather than trabecular compartment. There were limited associations between DXA-aBMD at central sites (lumbar spine and hip) and HR-pQCT parameters at both the distal tibia and radius. Nevertheless, some significant correlations were found between DXA-aBMD at the hip (femoral neck and/or total femur) and several trabecular HR-pQCT parameters at the distal tibia.
Conclusion: In adults with OI, there is initial evidence of site-specific agreement between DXA and HR-pQCT in the measurement of BMD values. Moreover, HR-pQCT may be able to provide information on bone quality that complements DXA evaluation at central sites. Additional patients will be included in this ongoing study, to validate our preliminary results and clarify the potential role of HR-pQCT in the characterisation of bone fragility in OI.
P125 Short-chain fatty acids (SCFAS) enhances bone health in postmenopausal osteoporosis A. Bhardwaj 1, L. Sapra1, R. K. Srivastava1 1All India Institute of Medical Sciences (AIIMS), New Delhi, IndiaObjective: Short-chain fatty acids (SCFA), the primary metabolites produced by intestinal microbiota, have an impact on both innate and adaptive immunity. It has been demonstrated that high fiber diet, the primary fermentable source of SCFA, reduces the degeneration of bone in rheumatoid arthritis. Based on these facts we were interested in investigating the effect of SCFAs (acetate, propionate and butyrate) in regulating bone health in postmenopausal osteoporosis (PMO). We aimed to investigate the role of SCFAs on bone health under estrogen-deficient conditions.
Methods: In vitro assays for osteoclastogenesis and osteoblastogenesis in the presence and absence of different concentrations of SCFAs were performed. Coculture assays of SCFAs primed Treg along with osteoclast/osteoblast were done to assess the immunoporotic potential of SCFAs. To further evaluate the mechanism of probiotics-induced prevention of bone loss in vivo, female C57BL/6 mice were randomly divided into the following groups viz. Sham, ovx (ovariectomized), ovx + probiotics (L. rhamnosus, and B. longum-109 CFU/d). At day 45 mice were sacrificed and bones (SEM, μCT); small intestine, large intestine, bone marrow, and mesenteric lymph nodes (flow cytometry); serum and fecal content (ELISA and HPLC) were harvested to assess the immunomodulatory role of SCFAs on ovx-bone loss.
Results: Ovariectomized condition led to enhanced bone loss in female mice as confirmed by SEM and µCT data. HPLC data showed that ovx mice had significantly lower fecal SCFA levels than the sham group, thereby confirming the potential role of SCFAs in regulating bone health. Next, we investigated the mechanism underlying SCFAs-modulation of bone remodeling via various in vitro assays. We observed that SCFAs significantly inhibit osteoclastogenesis along with promoting osteoblastogenesis in a dose-dependent manner. Furthermore, SCFAs were found to enhance the differentiation of Tregs significantly. Interestingly co-cultures of SCFAs primed Tregs with BM-osteoclast precursors inhibited osteoclastogenesis along with simultaneously enhancing osteoblastogenesis. Lastly, we confirmed that probiotics such as L. rhamnosus and B. longum prevent bone loss by restoring the level of SCFAs in ovx mice.
Conclusion: Altogether, our results for the first time propose SCFAs as potent regulators of bone health under ovx conditions thereby offering a mechanistic link between the “gut-immune-bone” axis. Our results have immense clinical implications in proposing the therapeutic potential of SCFAs in managing bone loss under osteoporotic conditions in the clinics.
P126 Risk groups for low vitamin d: changing the paradigm in clinical practice A. Bleizgys 1 1Vilnius Univ., Faculty of Medicine, Vilnius, LithuaniaIt is well established that musculoskeletal diseases, e.g., osteoporosis or rickets, can be caused by vitamin D insufficiency or deficiency. Therefore, those illnesses are considered risk factors for low vitamin D, i.e., such patients should be tested for their serum 25-hydroxyvitamin D levels that are the best marker of vitamin D status in clinical practice. However, there are many diseases and conditions that can themselves impair vitamin D metabolism, or dramatically increase requirements for this vitamin that cannot be met via natural sources (synthesis in the skin and from food). In addition, there’s some evidence that low vitamin D levels might contribute to the development of certain extraskeletal diseases. Clinicians should be familiar with the variety of risk factors that can help suspect low vitamin D in certain patients and, via vitamin D supplementation, replete their vitamin D stores, expecting improvement of at least the condition of musculoskeletal system.
P127 Stress factors in systemic lupus erythematosus (SLE) and antiphospholipid syndrome (APS) patients comparison A. Borisova 1, T. Lisitsyna1, D. Veltischev2, T. Reshetnyak1, O. Seravina2, O. Kovalevskaya2 1V.A. Nasonova Research Institute of Rheumatology, 2Serbsky NMRC PN MoH, Moscow, RussiaObjective: Stress factors in childhood and in a period before the manifestation of SLE and APS symptoms predispose and precipitate the development of rheumatic diseases. We aimed to describe predisposing and precipitating stress factors in SLE and APS patients.
Methods: 181 patients: 69 with SLE (60 women and 9 men), 55 with SLE and secondary APS (40 women and 15 men) and 57 with PAPS (37 women and 20 men), the median age of which was 31.0 [22.0; 41.0], 40.0 [32.0; 48.0] and 41.0 [35.0; 46.0] years, respectively, were consecutively enrolled in the study. Stress factors were detected by psychiatrist in semistructured interview in accordance with ICD10.
Results: Early childhood stressors were detected significantly more often in patients with SLE compared to PAPS and SLE + APS: 53 (76.8%) vs. 31 (54.4%), p = 0.006 and vs. 33 (60.0%), p = 0.03, respectively. Childhood stressors are also more typical for patients with SLE than PAPS: 55 (79.7%) vs. 36 (63.2%), p = 0.03. In particular, SLE patients were exposed to parental deprivation significantly more often than patients with SLE + APS (54 (78.3%) vs. 34 (61.8%), p = 0.04) and PAPS (54 (78.3%) vs. 32 (56.1%), p = 0.007); and also—a threat to safety in childhood was more common in SLE compared with PAPS (10 (14.5%) vs. 1 (1.75%), p = 0.01) and in adolescence compared with SLE + APS (11 (15.9%) vs. 2 (3.64)%), p = 0.02) and with PAPS (11 (15.9%) vs. 3 (5.26%), p = 0.05). Among childhood traumas, chronic stress factors predominated in patients with SLE: 60 (86.9%) vs. 34 (59.6%), p = 0.0005 in patients with SLE compared with PAPS and 40 (72.7%) vs. 34 (59.6%), p = 0.04 in patients with SLE + APS compared with PAPS. Stressful events at the onset of SLE were detected in 69.6%. At the same time, in patients with SLE + APS, chronic (18 (51.4%) vs. 12 (25.0%), p = 0.01) family stress predominated (17 (48.6%) vs. 10 (20.8%), p = 0.008), and in patients with SLE—acute stress (34 (70.8%) vs. 15 (42.9%), p = 0.009), including losses (7 (14.6%) vs. 0, p = 0.02). Multiple significant stressful events (cumulative stress load) before rheumatic disease were noted significantly more often in patients with SLE compared to patients with PAPS (32 (46.4%) vs. 13 (22.8%), p = 0.005) and SLE + APS (32 (46.4%) vs. 14 (25.5%), p = 0.01). Stressful events at the onset of APS were observed in 56.4% of patients. In patients with PAPS, acute stress situations prevailed compared with SLE + APS (23 (74.2%) vs. 14 (48.4%), p = 0.03), and in patients with SLE + APS, compared with PAPS, chronic (16 (51.6%) vs. 7 (22.6%), p = 0.02).
Conclusion: Compared with APS, SLE patients were more often exposed to stressors in childhood. At the same time, stressful events in childhood in patients with SLE were more often chronic. More than 2/3 of SLE patients and slightly more than half of APS patients experienced stressful event within a year before the onset of the disease. Multiple stressful events were observed in SLE patients much more often than in APS patients during life before the disease. The stress related predisposition and chronic stress precipitation could be a common pathogenesis factors for the development as the rheumatic disease, as the anxiety-depressive spectrum disorder, diagnosed in most SLE and APS patients.
P128 Patient and public involvement (PPI) in musculoskeletal research: a pragmatic review with resources for optimizing integration of patient experience data (PED) A. Botto-Van Bemden 1, A. Arumugam2 1Patient and Public Involvement, Musculoskeletal Research International, Inc., Miami, USA, 2Univ. of Sharjah, Dept. of Physiotherapy, Sharjah, United Arab EmiratesObjective: Patient and public involvement (PPI) is essential for Patient-Centered care and Patient-Focused Medicines Development. Proper PPI ensures optimal integration of Patient Experience Data (PED), helping to ensure patients’ expectations, needs and preferences are met. It is essential to ensure competence of the research team by capacity building with available tools and resources on PPI. This brief review aims to prompt PPI access and action by briefly summarizing the most relevant PPI resources.
Methods: This pragmatic review summarizes the most relevant best practices, checklists, guidelines and tools for optimizing PPI in musculoskeletal research. Practical resources for PPI in various stages of research projects are reviewed- conception, co-creation, design (including qualitative or mixed methods), execution, implementation, feedback, authorship, acknowledgement and remuneration of patient research partners, and dissemination and communication of research findings.
Results: A resource table with links to various tools and referenced material for PPI in various stages of research was created.
Conclusion: Gaps in research and challenges in care management create PPI opportunities for researchers and patient research partners (PRPs) to co-create meaningful studies and/or research development programs by setting research priorities together, developing protocol designs and research partnerships that are fit for purpose, improving recruitment and research awareness, team competence and capacity building, dissemination and sharing of results, actionable insights for improved access and regulatory approval, etc. Successfully optimizing integration of PPI research opportunities will require a shift in mindset for most and capacity building for all stakeholders.
Acknowledgement: We thank each patient partner for their contributions creating PPI tools and resources and all PPI stakeholders who encouraged and continue to encourage patient partnership.
P129 Therapeutic rehabilitation strategies in rheumatological syndromes in the neoplastic patient A. Bumbea 1, R. Traistaru1, V. Caimac1, O. Rogoveanu1, A. Musetescu1 1Univ. of Pharmacy and Medicine of Craiova, Craiova, RomaniaObjective: To establish a strategy to approach the neoplastic patient with rheumatoid syndrome.
Methods: Some nonspecific rheumatoid syndromes (1) can be secondary to a neoplastic pathology. Malignancy can determine multiple paraneoplastic phenomena, the substrate being chronic inflammation and the procoagulant status, the latter can also produce a stroke (2). We included a number of 20 patients (2013–2023) who presented with clinical aspects of rheumatoid arthritis or lupus-like syndromes secondary to a diagnosed neoplasia. The evaluation of these patients highlighted specific rheumatoid clinical aspects, moderate inflammatory biological syndrome. The rehabilitation consisted in the application of TENS on selected areas, as therapy allowed for the neoplastic patient. They were evaluated initially and at 3 months using the VAS scale and the ADL scale. All patients received combined anti-algesic therapy such as paracetamol, NSAIDs and recovery therapy.
Results: Patients with combined therapy showed a 31.4% reduction in rheumatoid syndrome with improved functionality. Biological tests were slightly influenced, but functionality improved by an average of 39.3%. The evaluation at 3 months maintained the same results.
Conclusion: The combined therapy of analgesics, low doses of nonsteroid and TENS therapy brings improvements in the quality of life of neoplastic patients with rheumatoid syndrome.
References:
1.De Cock D, Hyrich K. Best Pract Res Clin Rheumatol 2018;32:869
2.Bumbea AM, et al., Rom J Morphol Embryol 2017;58:1477
P130 The complex therapeutic approach of the painful shoulder in the stroke patient using rehabilitation techniques and botulinum toxin A. Bumbea 1, R. Traistaru1, V. Caimac1, A. Turcu Stiolica1 1Univ. of Pharmacy and Medicine of Craiova, Craiova, RomaniaObjective: To develop a complex therapeutic plan that includes the injection of botulinum toxin into the spastic muscles and a rehabilitation program for the painful shoulder in the patient with stroke and spasticity.
Methods: It is known from the literature that patients with spasticity benefit from botulinum toxin therapy, which allows the application of rehabilitation programs with superior results (1). Thirty patients with stroke and spasticity of the upper limb who presented pain and limited mobility at the shoulder level were studied. The patients were evaluated using the VAS scale, the Ashworth spasticity scale, and functional assessment of the shoulder. All patients received specific rehabilitation treatment, ultrasound applications, massage and physical therapy. The group was divided into two groups, Group A, which included 15 patients who received botulinum toxin treatment for spastic shoulder muscles. Group B received only rehabilitation treatment.
Results: It was found that group A that received botulinum toxin had a favorable functional evolution and a reduction in pain quantified on the VAS scale with a reduction of approximately 43.6%, compared to group B where the improvement was only 19.45%.
Conclusion: Spasticity therapy with botulinum toxin applied to patients with spasticity combined with upper limb rehabilitation program and shoulder pain had a much improved evolution.
Reference: (1) Bumbea AM, et al. Life Basel 2023;13:2218
P131 Comprehensive approach to the management and treatment of adults with X-linked hypophosphatemia (XLH) A. C. Polonsky 1 1Hospital Centenario, Rosario, ArgentinaObjective: X-linked hypophosphataemia (XLH) is an X-linked dominant disorder caused by mutations in PHEX1. XLH is the most common genetic form of hypophosphatemic rickets and osteomalacia. Its incidence has been estimated at 3.9–5 cases per 100.000 live births2. The mutations or chromosomal derangements affecting the phosphate regulating endopeptidase homolog, X-linked (PHEX) gene on the X chromosome lead to elevated levels of the hormone FGF23, resulting in renal phosphate wasting, impaired 1a-hydroxylation of 25-hydroxyvitamin D and consequently, chronic hypophosphatemia, impaired skeletal mineralization and rickets2. Patients usually develop clinical symptoms during the first or second year of life1. The clinical features include those common for hypophosphatemic rickets, short stature, waddling gait, and leg bowing in growing children, in addition to muscle weakness. Fatigue and chronic pain become more prevalent in older children and particularly adults2. Even adults with milder forms usually develop symptoms in their third or fourth decade, which may include bone and joint pain, fatigue, enthesopathy (commonly involving the hips and anterior spinal ligament), pseudofractures, dental complications and early osteoarthritis. These complications ultimately cause chronic pain, impaired mobility, loss of productivity and lower quality of life. Other complications include hearing loss, overweight and obesity has also been observed in XLH. The diagnosis of XLH relies on the combination of clinical, radiographic, biochemical and genetic features. Conventional management of XLH involves phosphate supplementation and active vitamin D (calcitriol). While conventional therapy can help manage bone pain, children with XLH can still develop significant lower limb deformity and often have short stature3. Burosumab is a neutralizing antibody to FGF23 and is superior to conventional management of the condition in both adults and children3. We aimed to evaluate the clinical and biochemical characteristics of a cohort of adult patients with XLH and evaluate the best therapeutic option.
Methods: A total of 11 adult patients were recruited, of which 8 had a diagnosis of XLH confirmed in childhood. The other two were diagnosed because they had a family member with the disease and a molecular study was performed to confirm the presence of XLH. Clinical follow-up, disease sequelae, laboratory, and therapeutic alternatives were carried out for one year. Only 8 of the 11 patients were evaluated until the end of the study.
Results: All the patients studied have a common characteristic of deformities in their limbs to a greater or lesser extent, decreased hearing, mostly mild, and dental disorders. Everyone complains of pain, both at rest and during movement. Only two patient underwent treatment without interruptions since childhood, but the majority stopped during adolescence. One of the patients, despite having had orthopedic surgeries in childhood and dental disorders, was diagnosed at the age of 64 years, also presenting postmenopausal osteoporosis, which is why we believe it is urgent to start therapy with burosumab. As seen in the Table, not all participants carried out the controls as established. From the results obtained, an increase in the phosphataemia value is evident in those patients who started with phosphorus salts but not in RTP. An increase in PTH is also evident as a consequence of conventional treatment.






Conclusion: Treatment for adults with XLH typically focuses on symptom management, including bone deformities and osteoarthritis. A multidisciplinary approach involving orthopedics, physiotherapy, and pain management is crucial for improving quality of life. Regular monitoring and adjustment of phosphate and vitamin D therapy are essential to maintain optimal levels and prevent complications. Burosumab, a monoclonal antibody approved for XLH treatment, has generally positive feedback. The problem with burosumab in my country is that it is so expensive, which can pose challenges for patients in terms of accessibility and affordability. The medical team must evaluate the cost–benefit relationship. It's understandable that some adult XLH patients may experience fatigue or reluctance regarding ongoing medical care from childhood. The weariness from years of treatments and appointments can impact motivation to adhere to medical recommendations. In these cases, addressing patients' concerns and emotions is crucial. To improve treatment adherence in adult patients with XLH, it is crucial to implement strategies that facilitate the integration of the therapeutic regimen into their daily lives. Some suggestions include: continuous education, psychological support, simplification of the regimen, reminders and follow-up, family involvement, regular monitoring, treatment personalization. These combined measures can contribute to better treatment adherence in adult patients with XLH. It is essential to work collaboratively with the medical team and consider the preferences.
References
1.Haffner D, et al. Nat Rev Nephrol 2019:15:435
2.Laurent M, et al. Front Endocrinol 2021:12:641543
3.Schindeler A, et al. Front Endocrinol 2020;11:338
P132 Comparative performance of CNN models in detecting fractures in x-ray images A. Chatsirisupachai 1, P. Nonthasaen1, P. Achararit1 1Princess Srisavangavadhana College of Medicine, Chulabhorn Royal Academy, Bangkok, ThailandObjective: This research confronts the public health challenge posed by osteoporotic fractures by comparing the effectiveness of convolutional neural networks (CNNs) in image classification vs. object detection tasks. We aimed to elucidate which method is more effective for fracture detection, which is critical in assessing fracture risk in osteoporosis.
Methods: We employed a FracAtlas dataset [1] with 717 abnormal scans out of 4,083 x-ray images. To achieve a balanced representation of fracture cases, 200 images with fractures and 200 without were designated for testing and validation, respectively. Classification models included MobileNetV3, Xception, and EfficientNetV2M, while object detection was performed with three variants of YOLOv8. For object detection, our evaluation criteria mirrored that of image classification—identifying at least one fracture correctly in an image was counted as a true positive, which aligns with clinical relevance where the detection of any fracture is the priority.
Results: Xception surpassed YOLOv8s in precision and F1-score, achieving 0.60 and 0.69, respectively, compared to YOLOv8s’s 0.49 and 0.65. However, YOLOv8m achieved a superior recall rate, suggesting a decision between these models hinges on specific requirements. Although classification methods don't pinpoint fracture locations directly, using visualization tools like Grad-CAM enhances fracture detection in classification tasks, providing an efficient alternative to the traditionally more labor-intensive object detection methods.
Conclusion: In a domain traditionally favoring object detection, our study uncovers the promising capabilities of image classification for fracture identification. It offers a streamlined, efficient approach to osteoporotic risk assessment, advocating for a paradigm shift in fracture detection methods. Image classification, enhanced with visualization techniques, stands out as a viable, resource-efficient option.
Reference: (1) Abedeen I, et al. Scientific Data 2023;10:521
Acknowledgement: This work was supported by Chulabhorn Royal Academy.
P133 Clinical and laboratory predictors of the development of chronic pain and early stages of PTSD osteoarthritis after knee injury A. Chernikova 1, A. Karateev1, M. Makarov1, E. Bialyk1, V. Bialik1, V. Nesterenko1 1Nasonova Research Institute, Moscow, RussiaObjective: Chronic pain and post–traumatic arthritis are frequent complications of injuries that cause suffering, loss of function and disability. To date, no clear predictors of the development of these complications have been identified. We aimed to determine the clinical and immunological factors associated with the development of chronic pain and early stages of post-traumatic osteoarthritis after knee joint injury.
Methods: From August 2022 to January 2023, 100 people were examined at the V.A. Nasonova Research Institute, including 56 women and 44 men at an average age of 26.95 ± 11.64 y, with an average BMI of 26.95 ± 4.99, who suffered a knee joint injury with persistent pain for a month or more. All patients agreed to the study, which is confirmed by informed voluntary consent. The patients underwent a clinical examination, laboratory research methods (UAC, highly sensitive CRP) were performed. A questionnaire was conducted on the scales of HRSH, KOOS, HAQ, CSI, BPI, Pain DETECT, FACIT-F, FIRST, HADS, and an MRI examination was performed on a Philips, MULTIVA 1.5 T device.
Results: According to the results of the study, it was revealed that the pain when moving along the CRH was on average 5.21 ± 1.30, the pain at rest on the CRH was on average 1.72 ± 1.74, the night pain on the CRH was on average 1.55 ± 1.84. Functional impairment according to HRH was 4.44 ± 1.79. Assessment of knee joint function: KOOS total was 52.02 (13;87), KOOS symptoms 62.26 (4;56), KOOS pain 60.58 (25;92), KOOS activity 68.97 (22;100), KOOS sport 28.92 (0;95), KOOS quality of life 41.02 (0;100). The value on the Pain DETECT scale, which evaluates the presence of signs of neuropathic pain, averaged 6.26 ± 4.79. According to the FIRST questionnaire, the indicators are from 0–5 (on average from 0.93 ± 1.26), which indicates the presence of concomitant fibromyalgia in some patients. According to the CSI questionnaires, the average values were 23.55 ± 13.38. According to the catastrophization scale, 13.54 ± 11.20. According to the HADS scales assessing the level of depression and anxiety, the values were 4.37 ± 4.01-depression and HADS anxiety with values on average 5.42 ± 4. According to laboratory research methods, hemoglobin values averaged 116 ± 179 g/l. The level of ESRD was 0.2 ± 15.3 mg/l, and the level of ESR was 2 ± 23.
Conclusion: Some patients who have suffered a knee injury more than 1 month ago experience severe pain and have impaired joint function. In a number of patients, 26% (26 out of 100 people), of whom 18 are women, the remaining 8 are men, there are signs of neuropathic pain, central sensitization, increased BMI, psychoemotional disorders and fibromyalgia, which aggravates the course of the post-traumatic period. Patients with chronic pain after an injury need further follow-up to clearly identify predictors of the occurrence of this condition in order to predict the occurrence of post-traumatic osteoarthritis and the formation of correct treatment tactics.
P134 Upper limb orthopedic assessment in paraplegic and tetraplegic patients and clinical outcomes on the shoulder, elbow, wrist and hand A. Cliquet Jr. 1 1Dept. of Orthopedics, Rheumatology and Traumatology, Faculty of Medical Sciences, UNICAMP, Campinas, SP, BrazilObjective: Spinal cord injured individuals (SCI) do present joint lesions on their overused upper limbs, being wheelchair users and due to upper limb effort during daily activities such as transferring. This work aimed at providing an assessment on the orthopedic comorbidities as well as feasible approaches towards clinical improvements on the shoulder, elbow, wrist and hand.
Methods: MRI, disability of the arm, shoulder and hand (DASH) score, bone densitometry (DXA), plain radiography and clinical measurements such as active and passive range of motion were performed in patients attending the SCI Outpatient Clinic of the University Hospital, including those patients involved in Paralympic Sports. Rehabilitation protocols were applied.
Results: On the shoulder, 10% of the tetraplegic athletes (sample of 10 rugby players) did present tendinopathies against 30% of those sedentary ones (sample of 10 tetraplegics). Joint strength, endurance and function were improved (sample of 17 subjects) by protocols of the rehabilitation programme of specific physiotherapy training of the scapula muscles making use of elastic bands. Rugby training also improved bone mineral content in the arms. On the elbow joint, clinical and radiological abnormalities (osteoarthritis, subclinical acute and chronic pain) were noticed in SCI patients, assessed through bilateral X-ray exams, on 10 paraplegics and 10 tetraplegics, such comorbidities being more evident (90%) on the latter pathology. Related to wrist and hand, SCI patients (8 paraplegics, 6 tetraplegics) presented minimal radiological signs of osteoarthritis.
Conclusion: Regular wheelchair rugby enhances bone mass and sedentary tetraplegic individuals do present more risk of injury to the acromioclavicular joint. Elbow osteoarthritis, being a limiting disease to the patients, requires both, early diagnosis and treatment through rehabilitation techniques.
P135 Évaluation of bone mineral density in Algerian patients with plaque psoriasis: a case–control study A. Djebbari 1, A. Abiayed2, S. Bennedjma2, H. M. Houbi3, S. Oulebssir1, A. Beguiret3 1HCA Hospital Koubap, 2HCA Hospital, 3HCA Hospital, Kouba, AlgeriaObjective: Psoriasis is a common chronic skin diseases, causing plaques. It is associated with many comorbidities. A link had been found between psoriasis and osteoporosis in some studies where various mechanisms may be involved, including increased inflammatory cytokines, such as interferon-gamma, IL-6, and TNFs. Moreover, psoriasis medications could cause abnormal BMD, which is measured by DXA as a gold standard method. Because the poverty of literature on the subject and the conflicting results in previous studies, for the first time in Algeria, we conducted a study to assess BMD in plaque psoriasis patients compared with a healthy control group to Improve the management of comorbidities associated with psoriasis. Our objectives were to evaluate the BMD measured by DXA in Algerian patients presenting a plaque psoriasis and identify associated factors with low BMD.
Methods: In this case–control study, 90 participants were enrolled from Algiers and Blida dermatology clinics University Hospital in Algeria between October 2019 and April 2022. The case group consisted 48 patients aged 20–65 from healthy subjects referred to these clinics for routine examination. Patients with psoriatic arthritis, chronic inflammatory diseases, endocrine disorders, a history of treatment with systemic drugs affecting BMD (including corticosteroids, disease-modifying antirheumatic drugs (DMARDs), and biologic drugs), individuals undergoing phototherapy, and those with a history of smoking and alcohol use were all excluded from the study. All participants were examined and evaluated for height, weight, BMI, medication history, pelvic fracture history, and chronic diseases. DXA was used to measure BMD at the 2nd and 4th lumbar vertebrae and the pelvis, and the results were categorized by T-score. The psoriasis area severity index (PASI) score was used to determine the severity of psoriasis.
Results: This study was conducted on 45 patients with a mean age of 47.23 ± 8.11 and 45 healthy controls with a mean age of 49.26 ± 6.7 to assess the relationship between BMD and plaque psoriasis. The mean T-score in the case and control groups were − 0.56 ± 1.02 and − 0.25 ± 0.65, respectively (P = 0.325). The mean T-score had a significant inverse correlation with an age of 42 y or above (P < 0.001), disease duration of more than 6 y (P = 0.05), and PASI score (P < 0.001), but had a positive correlation with sunlight exposure (P < 0.001), and overweight (P < 0.001).
Conclusion: Our study revealed that in Algerian patients, the mean T-score in patients with plaque psoriasis was significantly lower than the controls among those aged 42 or above. Furthermore, T-score had a significant inverse relationship with age, disease duration, and PASI score, but a significant direct relationship with overweight and sunlight exposure, so in addition to routine therapy we suggest treatments given to this group of plaque psoriasis patients to prevent osteoporosis.
P136 Obesity is the most prevalent comorbidity in a newly diagnosed psoriatic arthritis population: Algerian cohort of dermatologic early detection A. Djebbari 1, S. Bennedjma2, S. Oulebssir1, A. Abiayed2 1HCA Hospital Koubap, 2HCA Hospital, Kouba, AlgeriaObjective: Psoriatic arthritis (PsA) is a heterogeneous disease with articular extra-articular disease features. PsA is associated with important comorbidities: cardiovascular, gastrointestinal, infectious, malignant, and psychiatric. However, they are less studied in PsA compared to other chronic inflammatory arthritis. The aim of this study is to describe the prevalence of comorbidities in PsA newly diagnosed among a population of psoriasis screened by the PURE4 questionnaire recruited dermatology clinics.
Methods: Between 2019–2022, a multicenter cross-sectional trial including patients selected in dermatology clinics using PURE 4 questionnaire, and a diagnosis of PsA confirmed by CASPAR criteria. Data collected: demographical, clinical (affected joints, axial involvement, enthesitis, dactylitis), biological, and treatment related. Data on comorbidities and risk factors were collected according to the EULAR recommendations on reporting comorbidities in chronic inflammatory rheumatic diseases in daily practice.
Results: In all, 43 PsA patients were included: 14 (33%) women, mean age ± standard deviation 50.76 ± 12.39 y, 44% of patients with PsA had psoriatic nail disease and scalp involvement seen in 37%. With reference to the PsA type, 30% patients presented with polyarthritis, 44% with oligoarthritis, 39% with enthesitis, dactylitis in 23% and 13% with axial arthritis. Most of them had low or moderate disease activity and 30% were taking a biologic. The most prevalent comorbidities were: obesity 18 (42%), dyslipidaemia 9 patients (21%), hypertension 7 (17%), diabetes 6 (14%) and ischemic heart disease 2 (4.65%). Cardiovascular events correlated with obesity (p < 0.001), smoking (p < 0.001), current moderate/severe psoriasis (p = 0.01) and PsA disease activity (p < 0.01). Regarding infectious comorbidities: 4 patients (9.3%) had a history of pulmonary infection, (4%) chronic viral hepatitis, of which 2 with B virus and 2 with C virus. One patient was diagnosed with neoplasia, but no correlation was identified with any of the clinical, biological or treatment related included variables. Only 4 patients (9.3%) were diagnosed with depression and 11.63% had inflammatory bowel disease.
Conclusion: PsA newly diagnosed is associated with a high prevalence of comorbidities, especially obesity and cardiovascular diseases. These comorbidities should be screened and taken into consideration in the therapeutic and management of PsA patients.
P137 Earlier age of psoriasis onset, high crp level at diagnosis and low educational level are associated with diagnostic delay in psoriatic arthritis A. Djebbari 1, A. Gouder2 1HCA Hospital Koubap, Kouba, 2Hmruc, Constantine, AlgeriaObjective: Psoriatic arthritis (PsA) is a chronic inflammatory disease characterized by cutaneous psoriasis, with peripheral and axial joint damage. Early diagnosis of PsA is important for improving long-term outcomes. Trends in diagnostic delay of PsA in Algeria (Africa) and factors associated with delay in diagnosis have not been well studied. Aims: (1) to determine the diagnostic delay in PsA in Algerian population from 2016–2022, and (2) to identify demographic and clinical characteristics associated with diagnostic delay in PsA.
Methods: We conduct a retrospective, population-based cohort of adult patients with PsA in Algeria from 2016–2022. All patients met the classification criteria. Diagnostic delay was defined as the time from any patient-reported PsA-related joint symptom to a physician diagnosis of PsA. Factors associated with delay in PsA diagnosis were identified through logistic regression models.
Results: 78 PsA were recruited from 2016–2022 with a physician or rheumatologist diagnosis. Mean (SD) age was 51.2 (14.8) y and 62% were male. Median time from symptom onset to physician diagnosis was 2.9 y (IQR 0.8–9.3). By 6 months, 10 (12.8%) received a diagnosis of PsA, 29 (37.1%) by 1 y, and 39 (50%) by > 2 y after symptom onset. No significant trend in diagnostic delay was observed over calendar time. Earlier age at onset of psoriasis symptoms (p < 0.0001), low educational level (p < 0.001) and higher CRP level were associated with a diagnostic delay of > 2 y, whereas patients with late onset psoriasis symptoms, high activity (PASI) were associated with a lower likelihood of delay.
Conclusion: Our study highlights that half of PsA patients had a diagnostic delay of > 2 y. Patients with younger age at psoriasis symptom onset, higher CRP level at psoriasis diagnosis or lower educational level before diagnosis were more likely to have a diagnostic delay of > 2 y, whereas patients with late onset psoriasis symptoms, high activity (PASI) were less likely to have a diagnostic delay.
P138 Comparison of the average daily production of vitamin D3 in Moroccan men between the summer and winter seasons A. E. El Maataoui 1, A. B. Belbo1, D. M. Dandan1 1IBN Zohr Univ. Faculty of Medicine and Pharmacy Agadir, Agadir, MoroccoObjective: Hypovitaminosis D is a global health problem, even in countries with abundant sunlight. Despite Morocco's geographical location, the prevalence of vitamin D deficiency and insufficiency is reported to be high. In men and women, the prevalence of vitamin D deficiency was 4.4% and 8.6%, respectively. Also, the prevalence of vitamin D (25(OH)D) insufficiency was 85.2% and 77.4% in men and women, respectively. The aim of this study was to estimate the average amount of vitamin D3 produced by sunlight exposure in Moroccan adult men during summer and winter, based on their everyday outdoor ultraviolet doses.
Methods: This is a prospective study that recruited male participants exclusively and was conducted in both summer 2022 and winter 2023. All participants were Moroccan and resided in the Agadir area of Morocco (30.428° N). The sample size was calculated using the formula for sample size: n = z2 × p(q)/d2. We included 324 men in the summer and 345 in the winter, all of whom were apparently healthy and from diverse socioeconomic backgrounds, ranging in age from 18–100 years old. Data were collected through a face-to-face interview questionnaire that assessed sun exposure variables for estimating the vitamin D3 produced by sunlight. The questionnaire also included sociodemographic and anthropometric variables, as well as medical history. The daily estimate of synthesized vitamin D3 was calculated using the following equation: estimate vitamin D3 (IU) per day = vitamin D dose (VDD) × (4900 IU) × skin type factor × fraction of body exposed × age factor.
Results: The study included participants aged 20–60, with 62.33% in the 20–40 age group and 23.31% in the 40–60 age group. Only 10.76% were over the age of 60. The majority of participants had Fitzpatrick skin type 3 (72.94%). During the summer period, vitamin D synthesis was below the recommended value of 600 IU/d for 0% of participants, between 600–1200 IU/d for 44.44% of participants, and ≥ 1200 IU/d for 55.55% of participants. During the winter period, 13.33% of participants had an average vitamin D synthesis below the recommended value of < 600 IU/d, while 74.20% had a synthesis between 600–1200 IU/d, and 12.46% had a synthesis of ≥ 1200 IU/d. The most important factors correlated with vitamin D production, in order of importance, are the amount of skin exposed to sunlight, the time of year, age, and duration of sun exposure.
Conclusion: In Moroccan men, the predictors of vitamin D3 production through sunlight exposure are the fraction of the body exposed, age, and season. These results do not correlate with the findings of Moroccan studies which have reported a high prevalence of vitamin D status insufficiency and the prevalence of vitamin D deficiency. All these studies used immunological techniques and not the reference technique for vitamin D determination.
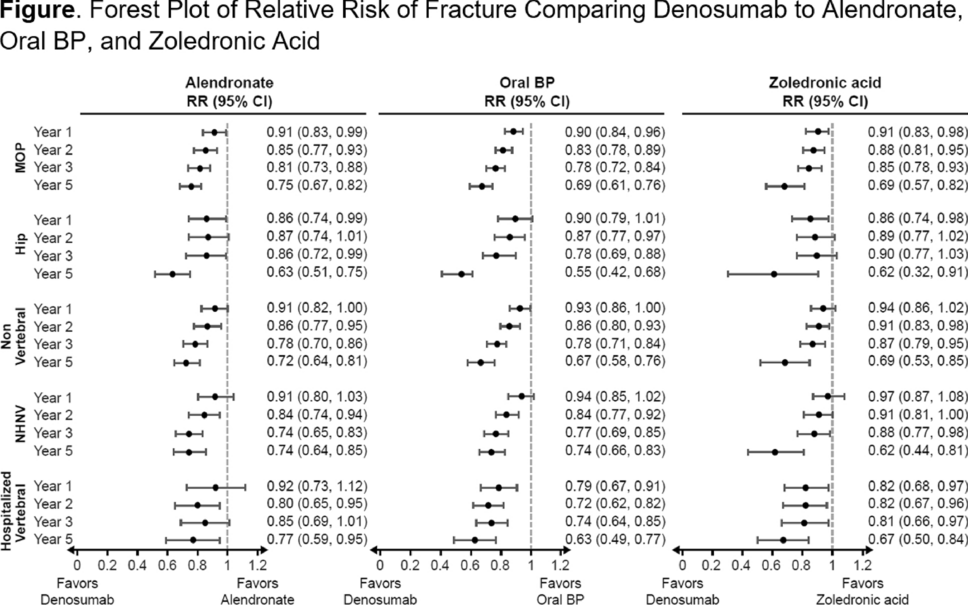
P139 once yearly zoledronic acid reduced the rate of new clinical fractures and improved survivalS. Z. Zidan1, A. E. Elsalmawy 2, M. M. Mouhsen2, I. M. Malik2, A. B. Butt.2 1North Middlesex Univ. Hospital, London, 2Southend Univ. Hospital, Southend-on-sea, UKObjective: Hip fractures are associated with high mortality and a substantial economic burden. Given its association with older age and the rate of aging of the global population, hip fractures are likely to become even more frequent events to bring patients to healthcare systems worldwide,
Methods: In this study, 656 patients with a fragility hip fracture were treated in Southend University Hospital and North Middlesex hospitals between 2021–2022, the first group of 356 patients was assigned to receive yearly intravenous zoledronic acid (at a dose of 5 mg), and 300 patients did not receive it either due to low creatinine clearance, ongoing renal disease, or due to patient preference. The infusions were first administered during the admission after surgical treatment of a hip fracture. All patients (mean age, 80.2 y) received supplemental vitamin D and calcium. The median follow-up was 1 y. The primary endpoint was a new clinical fracture.
Results: The rates of any new clinical fracture were 8.6% in the zoledronic acid group and 13.9% in the second group, with a 35% risk reduction with zoledronic acid (P = 0.001); the respective rates of a new clinical vertebral fracture were 2.7% and 3.8% (P = 0.02), and the respective rates of new nonvertebral fractures were 7.6% and 10.7% (P = 0.03). In the safety analysis, 8 of 356 patients in the zoledronic acid group and 19 of 300 patients in the second group died. The most frequent adverse events in patients receiving zoledronic acid were pyrexia, myalgia, and bone and musculoskeletal pain. No cases of osteonecrosis of the jaw were reported, and no adverse effects on the healing of fractures were noted. The rates of renal and cardiovascular adverse events, including atrial fibrillation and stroke, were similar in the two groups.
Conclusion: An annual infusion of zoledronic acid during hospital admission after repair of a low-trauma hip fracture was associated with a reduction in the rate of new clinical fractures and improved survival.
P140 Does the quality of diet affect bone mineral density in patients with inflammatory bowel disease? A. E. Ratajczak-Pawłowska 1, A. Szymczak-Tomczak1, M. Michalak2, A. M. Rychter1, A. Zawada1, K. Skoracka1, A. Dobrowolska1, I. Krela-Kaźmierczak1 1Dept. of Gastroenterology, Dietetics and Internal Diseases, 2Dept. of Computer Science and Statistics, Poznan Univ. of Medical Sciences, Poznań, PolandObjective: Looking for an association between BMD and diet quality among IBD patients.
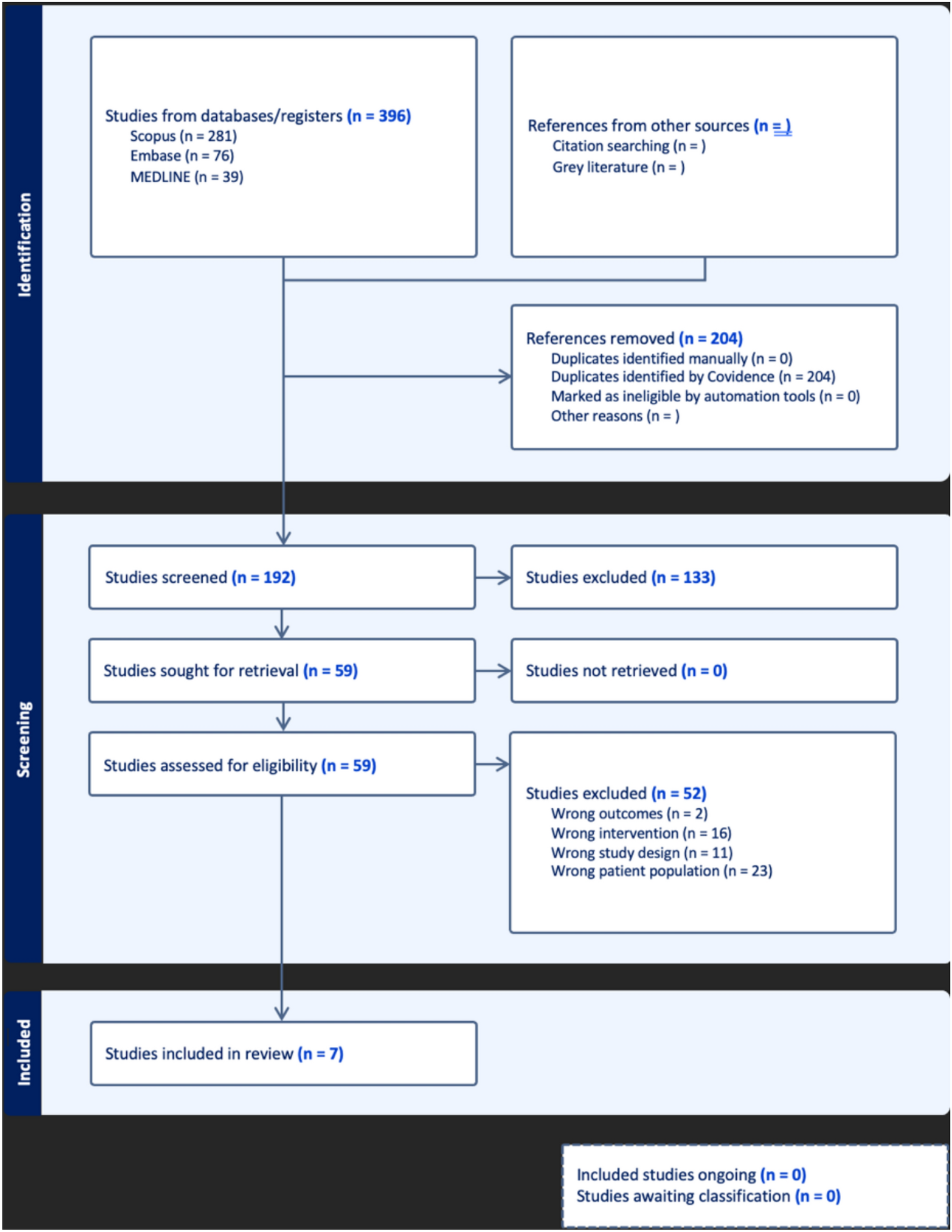
Methods: We enrolled 96 IBD patients (55 with Crohn’s disease—CD, 41 with ulcerative colitis—UC) and 33 healthy adults (control group—CG) at the age of 18–50, recruited at the Dept. of Gastroenterology, Dietetics and Internal Medicine, Poznan Univ. of Medical Sciences between 2020–2021. All subjects filled in the Questionnaire of Eating Behaviour (QEB), developed by the Polish Academy of Sciences, based on which pro-healthy and non-healthy diet indexes were calculated. Additionally, BMD, T-score and Z-score of the lumbar spine (L1–L4) and femoral neck (FN) were assessed using the Lunar DPX-Plus device (Lunar Inc., Madison, WI, USA). Finally, we carried out an appropriate statistical analysis. The summary of methods is presented in Fig. 1.

Results: Patients with UC and CD presented lower BMD, T-score and Z-score of L1–L4 and FN than the control group. Pro-healthy diet index was significantly higher among the control group than CD and UC. On the other hand, also non-healthy diet index was significantly higher among the control group than UC, but not CD. However, C-reactive protein concentrations were significantly lower among CG than CD and UC. We did not find differences between groups after dividing pro-healthy and non-healthy scores into low, medium and high categories. In the UC group, but not CD and CG, the pro-healthy index correlated positively with BMD, T-score and Z-score of L1–L4 and FN. Additionally, we find a positive correlation between non-healthy scores and BMI and body mass among UC patients. The summary is presented in the Fig. 2.
Comments (0)