This is the largest study to assess the CV safety of JAKis compared with anti-TNFα using clinical data from the WHO Global Drug Safety Database. The present data suggest that stroke, both fatal and non-fatal, may be the key event for the increased frequency of reported MACE seen with JAKis. Secondly, it suggests that the occurrence of these events in JAKi-treated patients is shorter than that in anti-TNFα-treated patients, supporting a real difference in their CV safety profile.
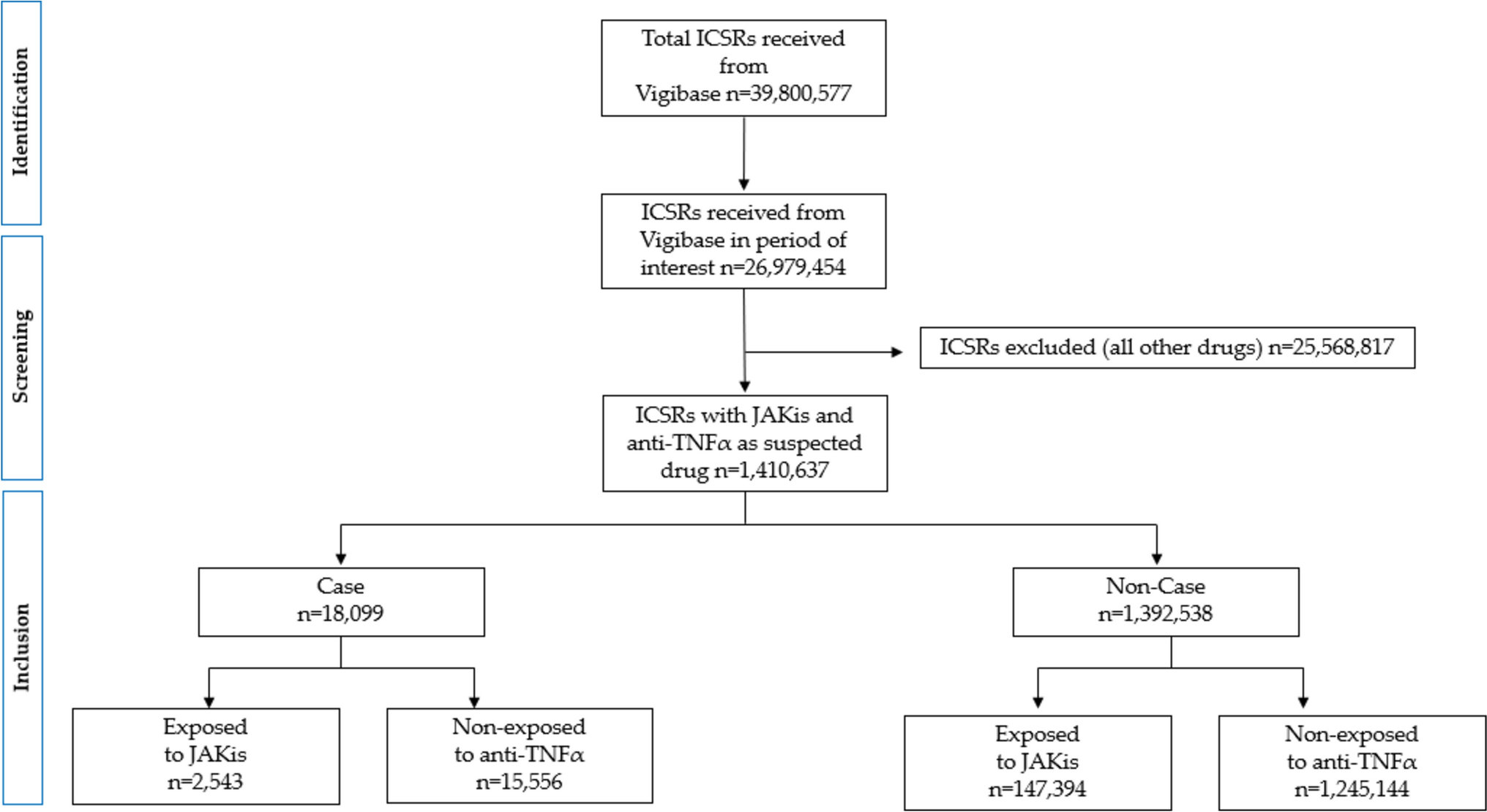
Although affected by the usual limitations of studies conducted in databases collecting ICSRs, several elements suggest that the results are reliable. First, among the exposed cases, JAKis were the only suspected drug in 71.9% of patients.
Second, the dataset did not include any reports collected after the FDA announcement, thus avoiding a notoriety bias either due to massive a posteriori reporting of cases that occurred before an alert (i.e., the seesaw effect) or because new events are relatively more likely to be reported after an alert than before [21]. Third, all sensitivity analyses showed comparable results to the main analyses. Fourth, the negative ROR for latanoprost supported the idea that these data may discriminate between drugs that can be associated with real reporting frequency and drugs that cannot.
The current study is the first to look at TTO for MACE and shows relevant differences between JAKi and anti-TNFα. MACE associated with JAKi tends to occur much earlier than with anti-TNFα (median TTO of 210 days vs 690 days), with lines of difference starting very early (around 30 days). However, as approximately 77.5% of reports do not provide this information, this analysis must be considered exploratory and these results should be interpreted with caution. Nevertheless, these results may be related to a real difference in the occurrence of MACE between JAKis and anti-TNFα, which merits further investigation.
A noteworthy finding from this study is that stroke emerged as a primary event among MACE. To date, there is a lack of studies comparing JAKis and anti-TNFα for each MACE event. One study with limited sample size and a very limited number of events did not reveal a difference between JAKis and anti-TNFα. It is thus likely to be too underpowered to be considered reassuring [22].
The mechanisms underlying the increased reporting of MACE or stroke are not well understood. Evidence in the literature suggests a possible increase in circulating lipid levels, which may induce atherosclerotic plaques [23]. JAKis may be associated with a small increase in low-density or high-density lipoproteins (LDL and HDL, respectively) [24], but this increase is of limited clinical relevance [25]. Furthermore, dyslipidemia is not a clear risk factor for stroke [26], especially in the short term.
Heart valve disease may also increase the risk of stroke and is a known potential long-term complication of RA. However, inhibition of the TNFα or JAK pathways appears to be protective [27, 28].
There may be an increased risk of atrial fibrillation in patients with RA [7]. To date, atrial fibrillation has not been recognized as an ADR of JAKi, although other protein kinase inhibitors may have off-target effects that can induce atrial fibrillation [29].
Another hypothesis is an increased risk of arterial hypertension. This is reported as common in the summary of product characteristics for tofacitinib, but not for etanercept, for example. Hypertension is probably the more relevant predictor of stroke [30], which may explain the results of the present study, both for stroke and for short TTO.
In the present study, although a slight majority of reports (49.9%) occurred in patients over 65 years of age, younger patients were found to be more frequent to report a MACE, which was quite unexpected. This could be due to reporting biases inherent in the reporting of ADRs, where, for example, a stroke occurring in a young patient after drug therapy may be more frequently suspected and reported as drug-related than the same event occurring in an older patient with other known risk factors. Furthermore, this result is not consistent with a recent study in which the hazard ratio for MACE was 2.06 (1.08–3.93) for those aged ≥ 65 years and 1.07 (0.60–1.89) for those aged < 65 years [8].
Regarding the potential frequency of reporting in patients aged ≥ 65 years, the confidence interval of the ROR for this age group is < 1, suggesting a lower frequency of reporting of MACE for JAKis compared with anti-TNFα in this population. However, this finding should be interpreted with caution due to the spontaneous reporting nature of the data, in which the unexpected events (e.g. MACE in the adult population) may be more frequently reported than the expected events (e.g. MACE in the elderly). Furthermore, it is important to emphasize that missing data on age are 4 times higher in ICSRs related to anti-TNFα than to JAKis, which may have influenced the results by age.
The gender differences observed in this study with regard to the incidence of MACE associated with JAKi are striking. While there was an increased frequency of reported MACE in both groups, men had a higher ROR compared with women. This finding suggests that while women have a higher prevalence of RA and are generally more frequent to report ADRs [31, 32], men may be more frequent to report MACEs associated with treatment with JAKi. This discrepancy may reflect gender-specific cardiovascular risk factors. Men have an inherently higher risk of cardiovascular disease, which may contribute to the higher reporting of MACE in this group [33].
Although all JAKis show an increased frequency of reporting MACE, significant differences in ROR between upadacitinib, baricitinib, and tofacitinib suggest that the frequency is not uniform within the class. In particular, upadacitinib has the highest ROR, followed by baricitinib and tofacitinib. The lack of a significant association with MACE for filgotinib further highlights that these differences may be due to the specific characteristics of each JAKi rather than a common class effect. Therefore, the variability in results suggests that each JAKi may carry different risks.
The results of the comparison between JAKis and anti-TNFα revealed a higher ROR when analyzing MACE events in Europe compared with the ROR obtained from all global MACE reports. This observation may be elucidated by potential variations in prescribing protocols, differences in patient characteristics compared with other countries, or increased attention of European prescribers before the PRAC risk reduction recommendation.
4.1 Strengths and Limitations
This study has some limitations. As with any other study based on reports mostly submitted voluntarily, its main weakness is underreporting; in routine pharmacovigilance, the reporting rate is on average 6% of the actual ADRs. However, a systematic review has shown that underreporting tends to be higher for non-serious ADRs, especially in general practice settings [34]. While the underreporting of serious ADRs remains significant, the impact on this work is likely limited since the case definition almost exclusively concerns serious cases. Nevertheless, it is likely that the present results underestimate the number of cases of MACE occurring in patients exposed to JAKis. On the one hand, while it is possible that clinicians’ attention to CV events may have influenced the number of reported cases to some extent compared with anti-TNFα, any particular attention to stroke was found prior to this study, which greatly reduces the possibility of a notoriety bias [21]. The potential for a notoriety bias was limited as much as possible by including only cases reported up to January 2023, the date of the EMA restriction on JAKi in elderly populations in European countries.
Another limitation is the incomplete data in the Vigibase ICSRs regarding the indication of use, such as RA, as these drugs are also used for other conditions. However, in order to reduce as much as possible the effect of different indications on the results of this study, the JAKis and anti-TNFα selected for this study were those that are primarily indicated in patients with RA.
An additional limitation of this analysis is the inclusion date for anti-TNFα, which was based on the first MACE report associated with tofacitinib in the VigiBase database, rather than the launch date of each drug. Although anti-TNFα agents were introduced before JAKis, this approach may have introduced some bias, as anti-TNFα agents were monitored for a longer period, whereas the reporting profile of JAKis may be more affected by the Weber effect [35]. In the context of the present disproportionality analysis, this choice could be considered conservative, as a potential Weber effect could relatively reduce the frequency of serious events, such as MACE, more for JAKis than for anti-TNFα, thus limiting the ability to detect significant differences in CV safety profiles between the two drug classes.
Another important limitation of this study, due to the nature of large observational data, is the inability to adjust for confounding factors such as severity of underlying disease. JAKis may be prescribed to a population with more severe disease compared with anti-TNFα, which could influence the observed results. Nevertheless, there is no apparent reason to believe that pre-existing CV risk factors could have influenced the choice of JAKis or anti-TNFα, particularly prior to the FDA or EMA communication.
The TTO analysis was based on < 22% of cases exposed to JAKis or anti-TNFα, thus reducing its absolute value. Nevertheless, the observed difference in median values is impressive and suggests a real difference between drug classes in the occurrence of MACE. Finally, the mechanism for the risk of CV events is not fully understood and a possible protective role of anti-TNFα should be considered.


Comments (0)