
Remember me
This non-interventional, retrospective register study was conducted in accordance with the Declaration of Helsinki and the Act on Secondary Use of Health and Social Data 552/2019, Finland. Study permission was granted by the Finnish Social and Health Data Permit Authority Findata (permission number THL/6325/14.02.00/2020). Ethical approval and written informed consents were not needed as the present study was based on secondary use of register data, as authorized by Findata in accordance with the Act on Secondary Use of Health and Social Data. The data included structured and unstructured data, were extracted from multiple registers/data sources by relevant data holders and were subsequently linked and pseudonymized by Findata. The linking of the data sets was based on unique personal identification numbers. All study analyses were performed on patient-level pseudonymized data, which were only available to authors who analyzed the data. The data were stored and analyzed in a secure operating environment provided and authorized by Findata. Results representing low patient numbers (< 5) to ensure patient anonymity and privacy were considered throughout the study.
The study population was identified based on electronic health records (EHR) of the public secondary healthcare centers of the hospital districts of Helsinki and Uusimaa (HUS) and Southwest Finland (HDSF). All hospital data were extracted from the data lake of each hospital, with data integrated from multiple EHR sources. Hospital data included demographics, inpatient medications, prescribed outpatient medications, contacts, diagnoses, procedures, pathology of tumor characteristics and electronic medical journals. Data on reimbursed outpatient drug purchases were extracted from the Social Insurance Institution of Finland. Dates and causes of death were retrieved from Statistics Finland.
Eligibility CriteriaThe study population included adult (≥ 18 years) incident female patients with EBC, as identified through an ICD-10 diagnosis code for BC (C50*) recorded in the specialty healthcare of HUS or HDSF between 1 January 2012 and 30 June 2019. Patients had to be residents within the HUS or HDSF regions at index. The index date was defined as the date of the first BC diagnosis recorded between January 2012 and June 2019. To exclude prevalent cases, a 2-year left censoring for prior BC diagnosis, and 90 days for prior BC drugs, before index was applied. The HR+/HR– BC subtype was defined utilizing data from ± 90 days from diagnosis. A patient was defined as HR+ based on pathology or if they had received endocrine treatment. HR+ was defined at a threshold of 1% when available in the pathology records or a mention of HR+ in the pathology text. If the pathology data were missing or inconclusive and there were no records of endocrine treatment, a patient was defined as HR status missing and excluded from the analyses. HER2 status was primarily based on in situ hybridization and, if unavailable, on immunohistochemistry (positive if 2+ , 3+). If the pathology data were missing or inconclusive and there were no records of anti-HER2 treatments, the patient was defined as HER2 status missing and excluded.
The BC stage [EBC vs. advanced BC (ABC)] was inferred based on radiological statements, recorded ICD-10 diagnosis codes, procedure codes and prescribed treatments. Individuals with de novo metastatic BC detected within 90 days from index were excluded.
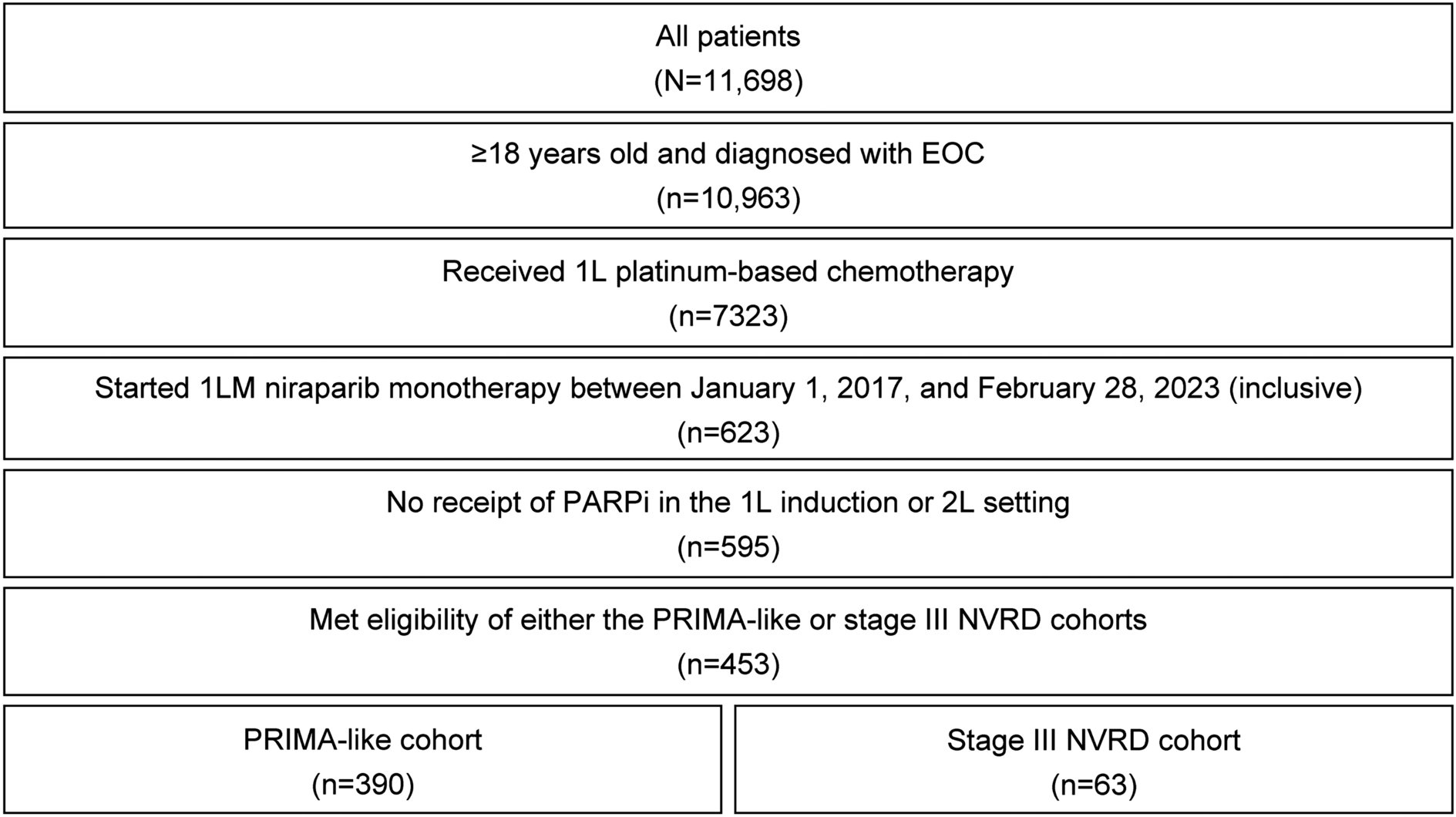
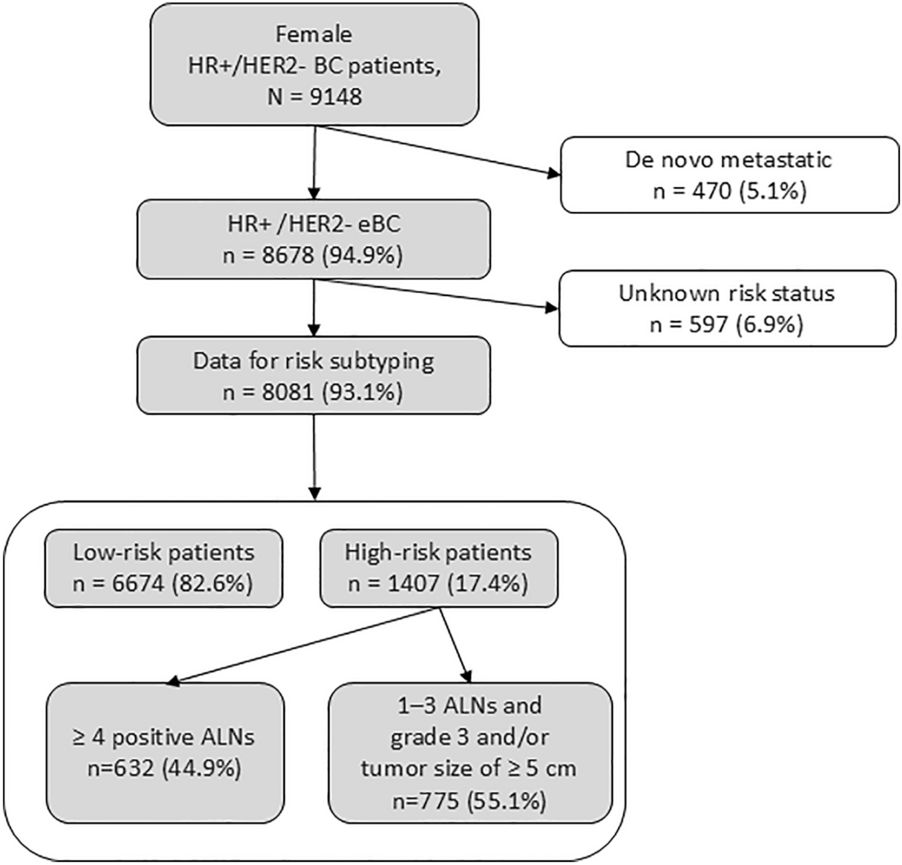
EBC Risk SubgroupsPatients were categorized into low- and high-risk HR+/HR– EBC subgroups based on clinicopathological criteria for high risk adapted from the monarchE trial cohort 1 population [11]. Patients with ≥ 4 ALNs or 1–3 ALNs with either grade 3 or primary tumor size ≥ 5 cm at index were classified as patients with high-risk EBC, while patients who did not meet the above criteria were defined as low-risk EBC. Individuals with missing ALN status information, or individuals with 1–3 ALNs who did not have any available information regarding either primary tumor size or grade, were defined as patients with unknown risk and were excluded from the main analysis (Fig. 1). Moreover, patients in the high-risk group were further stratified into two subgroups: patients with ≥ 4 ALNs and patients with 1–3 ALNs and primary tumor size ≥ 5 cm and/or grade 3.
Fig. 1
Cohort and subgroup formation. The present study assessed adult female patients with hormone receptor-positive, human epidermal growth factor 2 receptor-negative (HR+/HR–) early breast cancer (EBC) diagnosed in 2012–2019 in the Hospital District of Helsinki and Uusimaa (HUS) and the Hospital District of Southwest Finland (HDSF), Finland. Low- and high-risk subgroups were based on criteria from the monarchE trial cohort 1 high-risk population defined based on the number of axillary lymph nodes (ALNs), grade and tumor size [2]
Outcome MeasuresBC mortality was defined as death with BC reported as the immediate or main cause of death. IDFS and DRFS definitions utilized in clinical trials [11, 12, 18] were aligned with real-world data availability. IDFS included disease recurrence based on the detection of second primary non-breast cancer and/or re-initiation of chemo- or radiotherapy 1 year after BC diagnosis, initiated at least 3 months after prior chemotherapies, distant recurrence of metastatic disease and all-cause death. DRFS was defined as the time from index until distant recurrence of metastatic disease or all-cause death, whichever occurred first. The detection of metastases was based on mentioning of metastasis in free format texts within the medical charts, metastatic treatment, radiation therapy to non-breast site or procedure codes specific for advanced disease.
Time to Endocrine Treatment DiscontinuationThe time to ET discontinuation was based on the timing of tamoxifen and aromatase inhibitor purchases. Both neoadjuvant and adjuvant ET was included. Patients with a gap in ET purchases of > 12 months were considered to have discontinued treatment. Patients with purchases within 12 months before end of follow-up were censored. Death and distant relapse were considered competing outcomes as reasons for the treatment discontinuation.
Statistical AnalysisBaseline CharacteristicsData on comorbidities and Charlson comorbidity index (CCI) were collected up to 2 years prior to index. CCI was calculated according to Quan et al. [19] based on existing ICD-10 code records with the exception of breast cancer diagnoses. Categorical variables were compared between the low- and high-risk groups using chi-squared test.
IncidenceIncidence of high-risk HR+/HR– EBC was calculated based on the base population size, which was defined as the number of adult women alive in the HUS and HDSF regions at the end of each year during the study period, (data from Statistics Finland; in 2018, approximately 896,000 persons). Incidence across the entire study period (“Overall”) was derived by dividing the total number of patients diagnosed with HR+/HR– BC during the entire study period by the total base population size during the same period.
Outcome MeasuresIDFS, DRFS and OS probabilities were estimated using Kaplan-Meier survival analysis, with the survival estimates at 5 years accompanied by 95% confidence intervals (CI) and the number of patients at risk reported at 12-month intervals. All outcomes were censored at the end of study, 31 December 2019. Overall survival (OS) was analyzed as time from index until death of any cause. Competing risk analyses were run for BC mortality (BC death as event and other any cause of death as competing risk), DRFS (distant relapse as event and all-cause death as competing risk) and IDFS (distant relapse/disease recurrence as event and all-cause death as competing risk). Respective cumulative incidences were obtained with the Aalen-Johanssen estimates and plotted as a function of time with the 95% CIs.
Multivariable Cox proportional hazard (PH) model was adopted to evaluate OS by accounting for age, CCI [19] and risk group or number of ALNs, tumor size and tumor grade as covariates. The PH assumption was checked visually by plotting the Schoenfeld residuals. Cause-specific Cox PH models were used to examine the association of age, CCI and risk group or number of ALNs, tumor size and tumor grade with BC mortality, DRFS and IDFS, adopting a competing risk analysis for each outcome as described above. All Cox models were stratified by the region (HUS or HDSF). The hazard ratios (HRs) with 95% CIs and p-values were reported.
A p-value < 0.05 was considered statistically significant in all analyses. Missing data were not imputed, and the proportion of missing values were reported where feasible. Data handling and all analyses were conducted with the Statistical programming language R, version 4.0.3 [20].
Comments (0)